

Handling PDF files online is actually quite easy using our PDF tool. You can fill in Va Form 21 6898 here painlessly. The tool is continually updated by us, getting awesome functions and becoming better. With a few easy steps, you'll be able to start your PDF editing:
Step 1: Open the PDF file in our tool by clicking the "Get Form Button" in the top section of this page.
Step 2: Once you access the file editor, you'll notice the form all set to be filled out. Aside from filling in different blank fields, you might also perform other sorts of actions with the form, specifically writing any text, changing the original text, adding graphics, placing your signature to the form, and more.
This document requires particular information to be filled in, so ensure that you take some time to fill in exactly what is required:
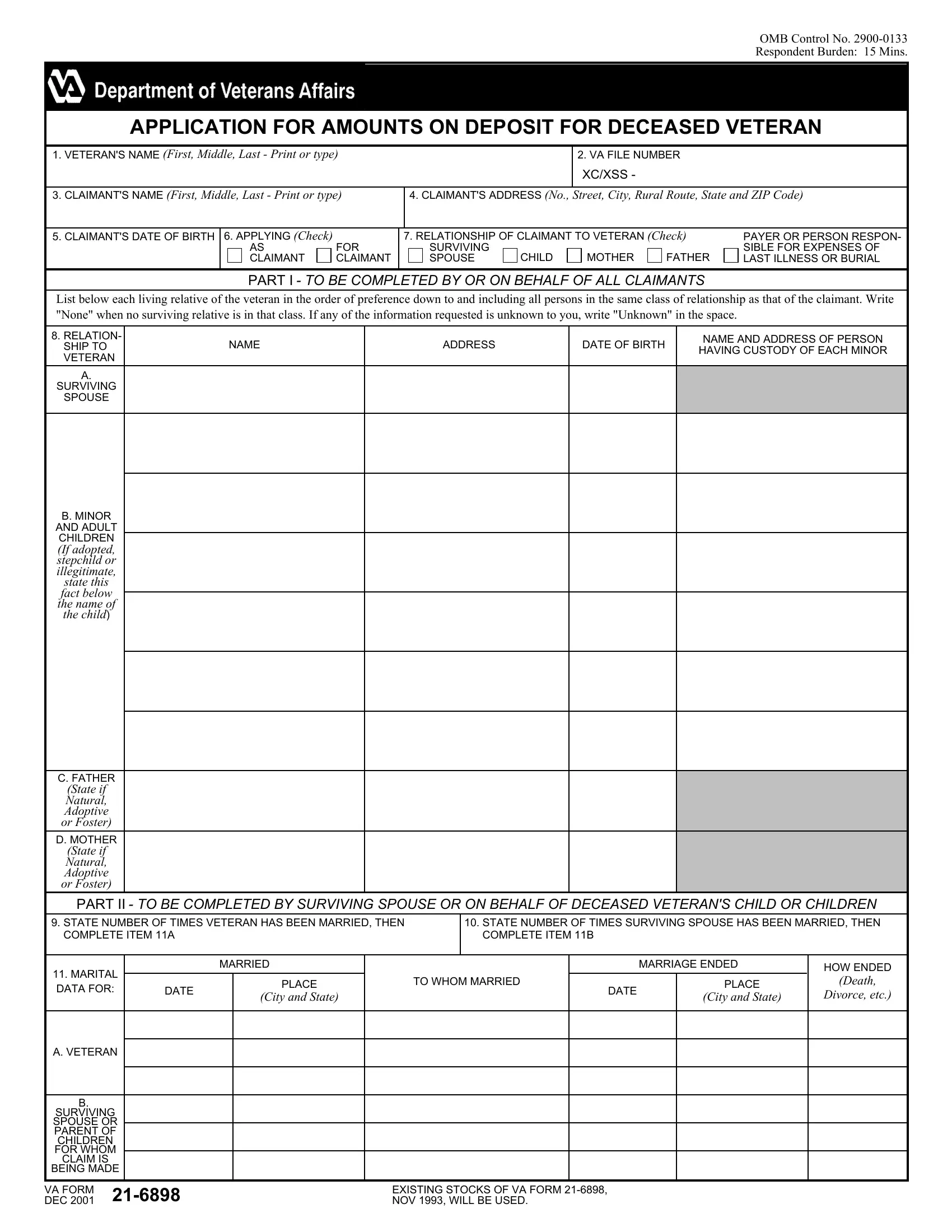
1. Start completing the Va Form 21 6898 with a number of essential blanks. Consider all the information you need and be sure not a single thing neglected!
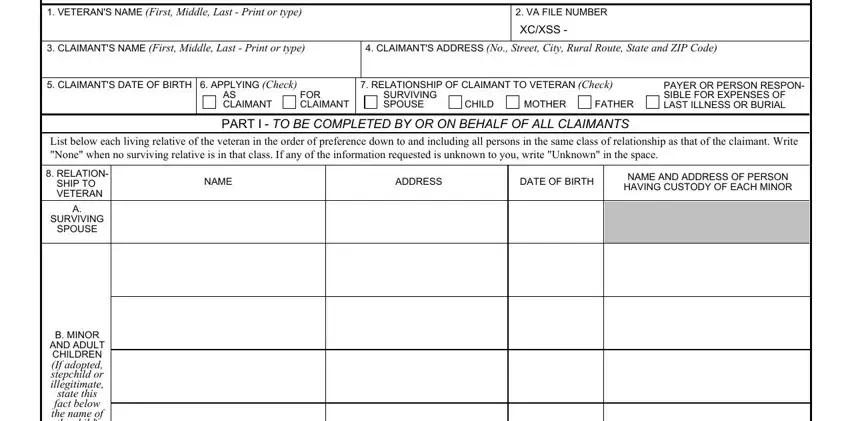
2. Once your current task is complete, take the next step – fill out all of these fields - state this fact below the name of, C FATHER, State if Natural Adoptive or Foster, D MOTHER, State if Natural Adoptive or Foster, PART II TO BE COMPLETED BY, STATE NUMBER OF TIMES VETERAN HAS, STATE NUMBER OF TIMES SURVIVING, MARITAL DATA FOR, DATE, MARRIED, PLACE, City and State, TO WHOM MARRIED, and MARRIAGE ENDED with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
You can easily make errors when filling out the DATE, so be sure to look again before you'll finalize the form.
3. In this stage, check out BEING MADE, SURVIVING SPOUSE OR PARENT OF, CLAIM IS, VA FORM DEC, and EXISTING STOCKS OF VA FORM NOV. Each one of these will have to be filled in with highest accuracy.

4. Now fill in this next part! Here you will have all these WAS VETERAN AT ALL TIMES A MEMBER, YES, If No explain fully giving reasons, A STOCKS BONDS BANK DEPOSITS ETC, B REAL ESTATE, C OTHER PROPERTY, D AMOUNT OF INDEBTEDNESS E NET, NET WORTH AT TIME OF VETERANS, AVERAGE MONTHLY INCOME OF YOUR, AVERAGE MONTHLY EXPENSES OF, INDICATE THE SOURCE FROM WHICH, SOURCE OF INCOME, AMOUNT, SOURCE OF INCOME, and AMOUNT fields to do.
5. When you near the completion of the document, you'll notice just a few more requirements that should be fulfilled. Particularly, WERE ANY PERSONS LIVING IN YOUR, YES, If Yes complete items below, NAME OF DEPENDENT, DATE OF BIRTH, RELATIONSHIP TO CLAIMANT, PART IV TO BE COMPLETED BY THE, BURIAL PROVIDED VETERAN WAS NOT, A PLACE OF VETERANS DEATH City and, B PLACE OF BURIAL City and State, C CLAIMANTS RELATIONSHIP TO VETERAN, NOTE ANSWER FULLY Each charge, NATURE OF, EXPENSE, and NAME OF PERSON OR FIRM RENDERING should all be filled out.
Step 3: Be certain that the information is correct and then click on "Done" to complete the project. Sign up with us now and instantly gain access to Va Form 21 6898, ready for downloading. Every last modification made is conveniently preserved , which enables you to customize the pdf at a later point as needed. FormsPal offers safe form tools with no personal information record-keeping or distributing. Feel safe knowing that your data is in good hands here!