
 CHILD
CHILD
Filling out documents along with our PDF editor is more straightforward when compared with most things. To modify va form 21p 8049 the form, there is little you have to do - just adhere to the actions listed below:
Step 1: The webpage includes an orange button stating "Get Form Now". Press it.
Step 2: You'll notice each of the options that it's possible to undertake on the file once you've entered the va form 21p 8049 editing page.
In order to fill in the form, type in the details the program will require you to for each of the appropriate sections:
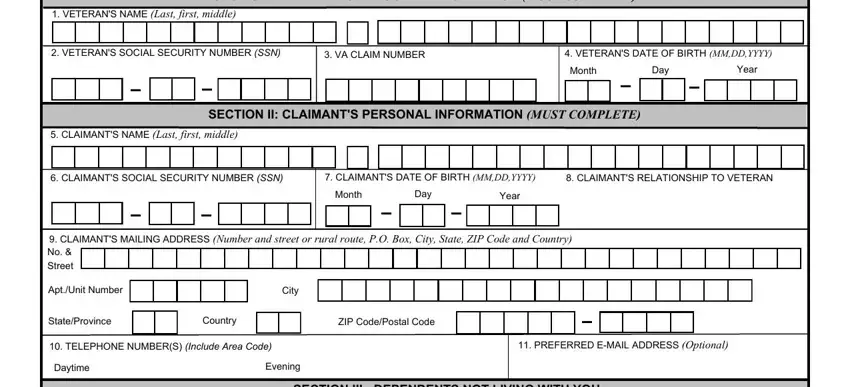
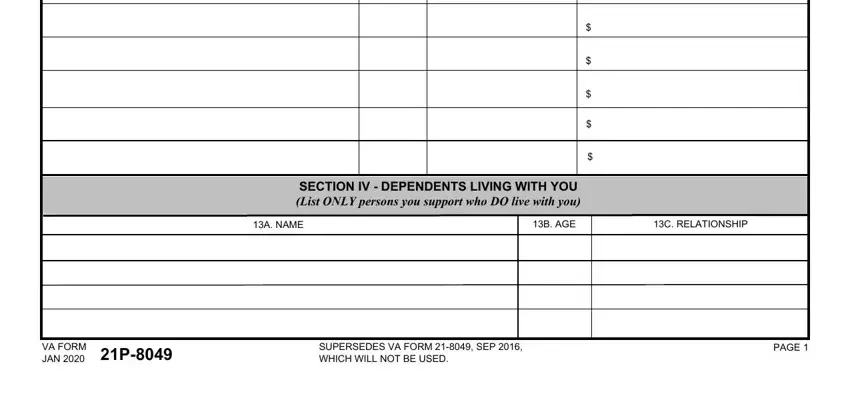
Feel free to type in your information in the field SECTION IV DEPENDENTS LIVING WITH, A NAME, B AGE, C RELATIONSHIP, VA FORM JAN P, SUPERSEDES VA FORM SEP WHICH, and PAGE.
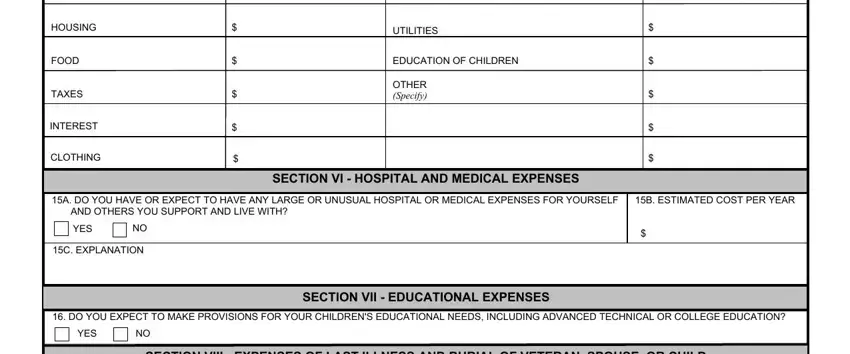
Jot down the significant particulars in A ITEM, B AMOUNT, A ITEM Continued, B AMOUNTContinued, HOUSING, FOOD, TAXES, INTEREST, CLOTHING, UTILITIES, EDUCATION OF CHILDREN, OTHER Specify, A DO YOU HAVE OR EXPECT TO HAVE, B ESTIMATED COST PER YEAR, and SECTION VI HOSPITAL AND MEDICAL segment.
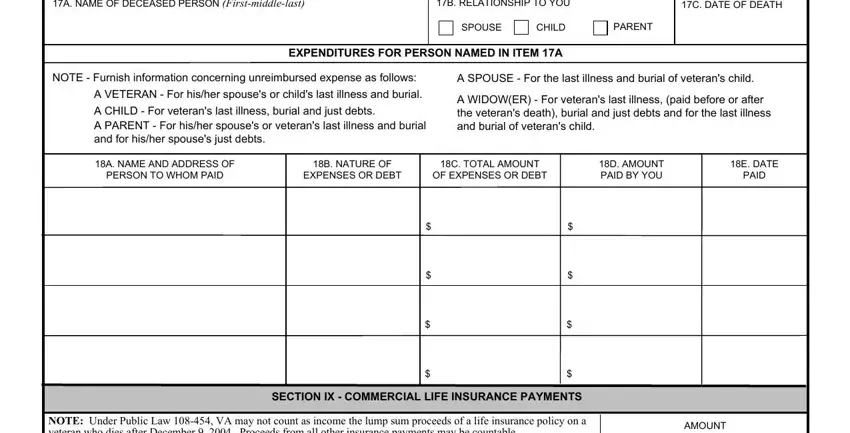
Please be sure to describe the rights and obligations of the sides inside the A NAME OF DECEASED PERSON, B RELATIONSHIP TO YOU, C DATE OF DEATH, EXPENDITURES FOR PERSON NAMED IN, SPOUSE, CHILD, PARENT, NOTE Furnish information, A SPOUSE For the last illness and, A VETERAN For hisher spouses or, A WIDOWER For veterans last, A NAME AND ADDRESS OF PERSON TO, B NATURE OF EXPENSES OR DEBT, C TOTAL AMOUNT OF EXPENSES OR DEBT, and D AMOUNT PAID BY YOU section.
Finish by taking a look at the next sections and filling them out as required: NOTE Under Public Law VA may not, TOTAL RECEIVED OR EXPECTED BY, EXPECTED OR ACTUAL DATE OF RECEIPT, NAME OF THE DECEASED FOR WHOM, VA FORM P JAN, and PAGE.
Step 3: Click the Done button to be certain that your completed document is available to be exported to each device you use or mailed to an email you indicate.
Step 4: To prevent yourself from any kind of difficulties as time goes on, you should create up to several copies of your document.
