This PDF editor was designed to be as simple as it can be. As soon as you keep to these actions, the process of creating the Va Form 21P 4706B file is going to be easy.
Step 1: Select the button "Get form here" to access it.
Step 2: So you're on the file editing page. You may enhance and add text to the document, highlight words and phrases, cross or check particular words, insert images, insert a signature on it, get rid of unneeded areas, or eliminate them completely.
These sections are what you are going to complete to receive the prepared PDF file.
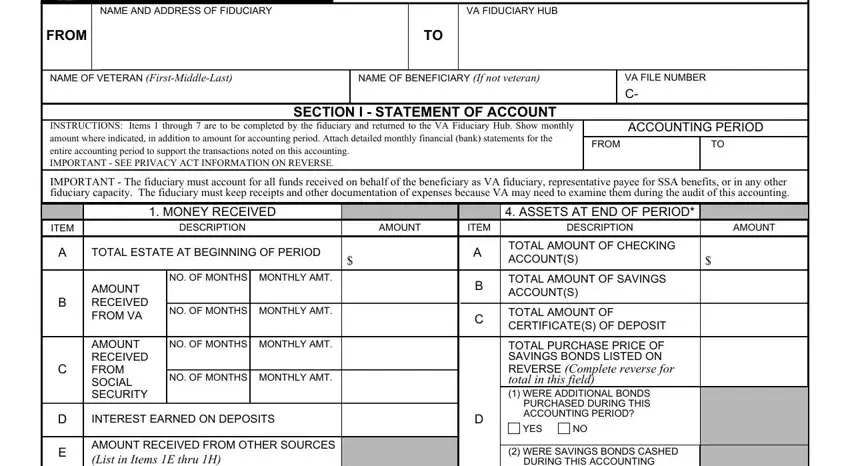
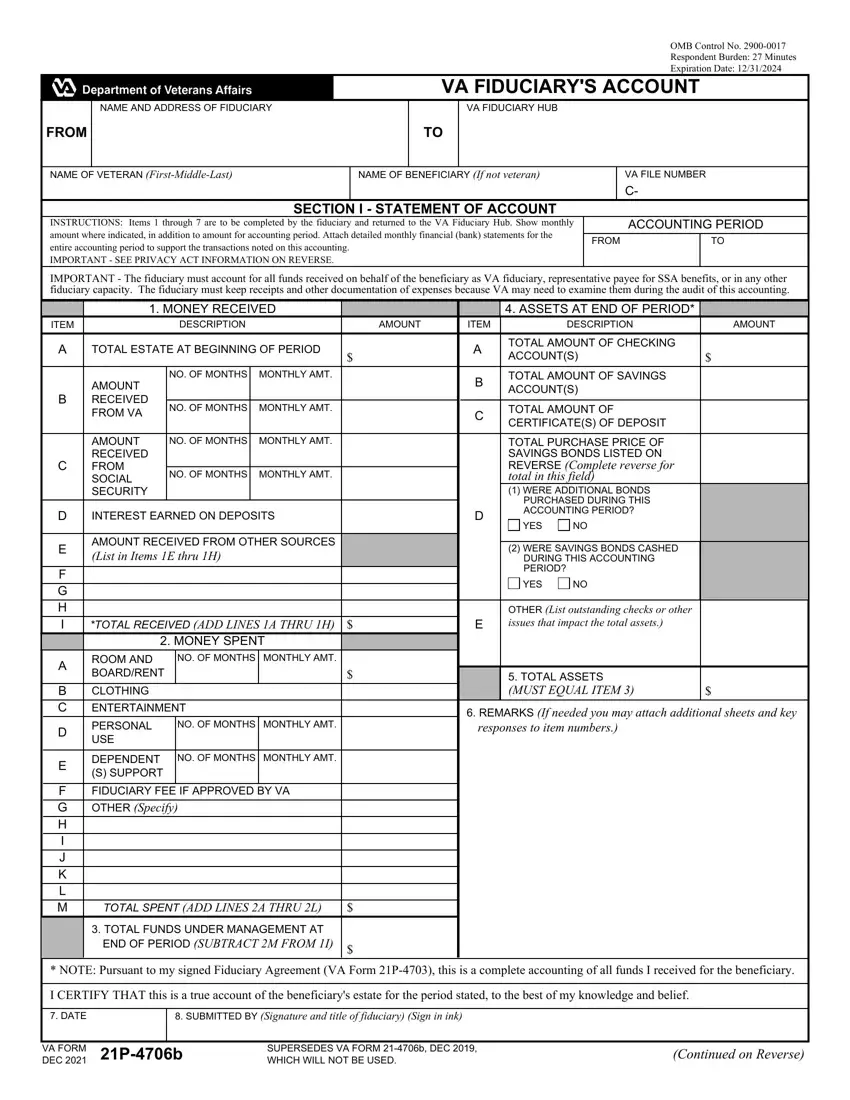
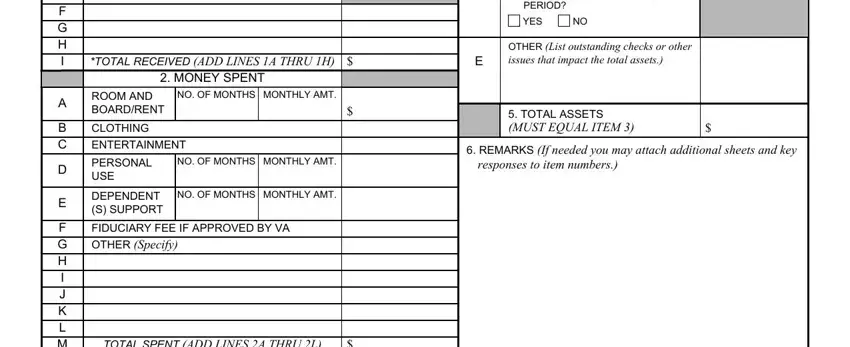
Type in the data in the F G H I, B C, F G H I J K L M, AMOUNT RECEIVED FROM OTHER SOURCES, TOTAL RECEIVED ADD LINES A THRU H, MONTHLY AMT, ROOM AND BOARDRENT, CLOTHING ENTERTAINMENT, PERSONAL USE, DEPENDENT S SUPPORT, NO OF MONTHS MONTHLY AMT, NO OF MONTHS, MONTHLY AMT, FIDUCIARY FEE IF APPROVED BY VA, and TOTAL SPENT ADD LINES A THRU L area.
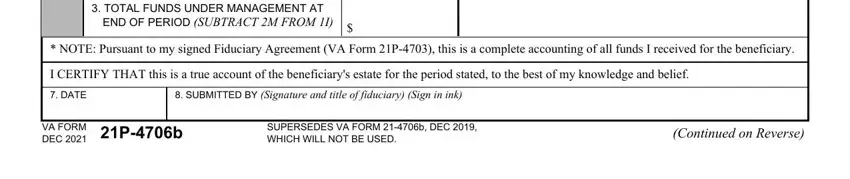
Note down any data you are required inside the area TOTAL FUNDS UNDER MANAGEMENT AT, END OF PERIOD SUBTRACT M FROM I, NOTE Pursuant to my signed, I CERTIFY THAT this is a true, DATE, SUBMITTED BY Signature and title, VA FORM DEC Pb, SUPERSEDES VA FORM b DEC WHICH, and Continued on Reverse.
The I certify that during this, I certify that during this, EXPLANATION OF BACKGROUND, LINE NO, SERIAL NUMBER, DATE OF PURCHASE, PURCHASE PRICE, LINE NO, SERIAL NUMBER, DATE OF PURCHASE, and PURCHASE PRICE field will be your place to include the rights and obligations of all parties.
Finish the file by looking at these particular fields: SECTION II CERTIFICATION OF US, SIGNATURE OF FIDUCIARY Sign in ink, DATE, PRIVACY ACT INFORMATION The VA, RESPONDENT BURDEN We need this, and VA FORM Pb DEC.
Step 3: After you've selected the Done button, your document is going to be readily available transfer to any kind of gadget or email address you identify.
Step 4: You can also make duplicates of the document tokeep away from different possible issues. Don't be concerned, we do not disclose or record your data.
