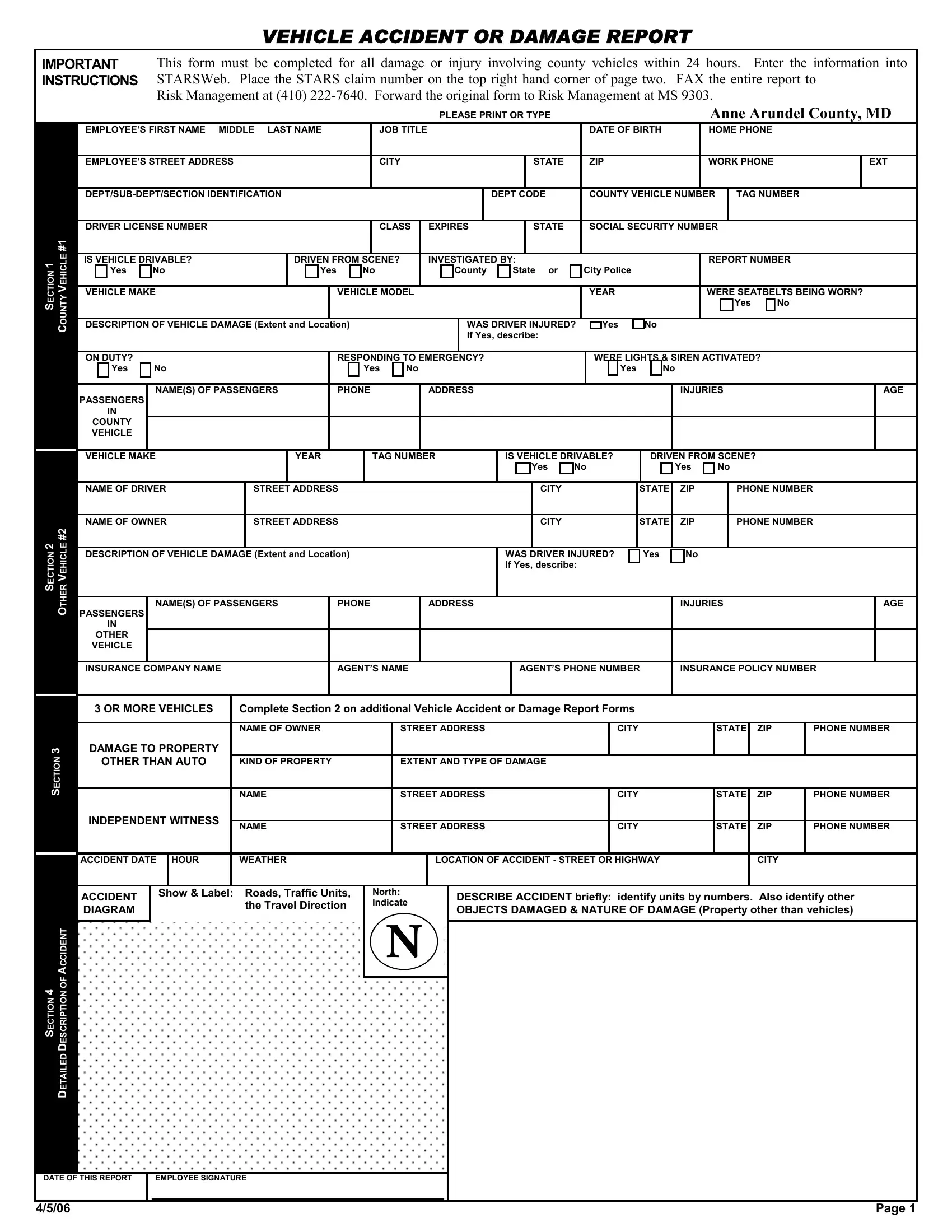

A vehicle accident report template is essential for all insurance company claims, legal matters, and internal reviews. Below is a step-by-step guide on how to complete this form correctly.
1. Basic Info and Vehicle Identification Number
Start by filling out the basic information for the employees and vehicle. Include the employee's name, driver's license, job title, department, contact details, vehicle make, model, year, and tag number. This data sets the context for the report.
2. Document the Accident Details
Record details about the accident, such as the date when the crash occurred, time, and location. Note the weather conditions and note whether the vehicle was driven from the scene. Include a diagram of the accident layout to provide a clear visual understanding of the incident.
3. Describe Vehicle Damage and Injuries
Detail the extent and location of the vehicle's damage. If there were any injuries to the driver or passengers, describe these as well. Confirm whether seatbelts were worn and if the vehicle was drivable post-accident.
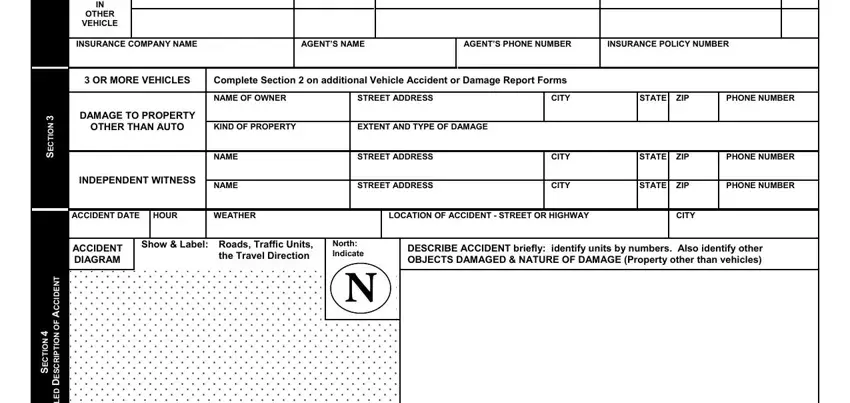
4. Witness Information for Insurance Company
If there were any witnesses to the crash or incident, record their names, phone numbers, and addresses. Witness accounts can be crucial for insurance and legal purposes.

5. Report on Law Enforcement Involvement
Indicate whether the accident was investigated by local, county, or state police and include any relevant report numbers. This information may be necessary for official records and proceedings of the traffic accident.
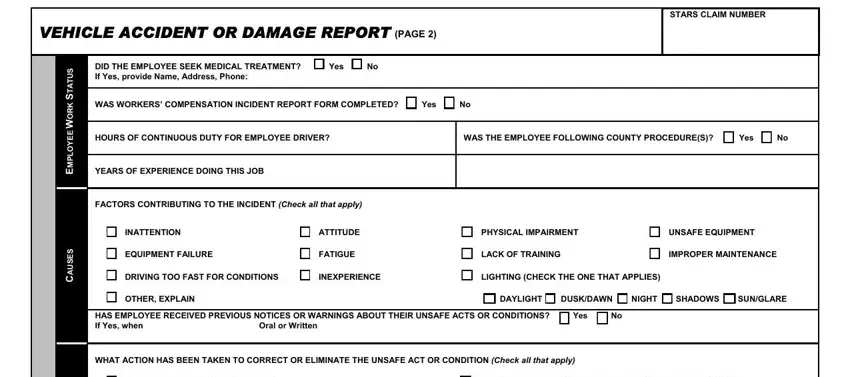
6. Include Additional Information
Fill out any additional relevant sections such as damage to other property, involvement of other vehicles, and any post-accident measures, like the person seeking medical treatment or the status of a workers' compensation claim.
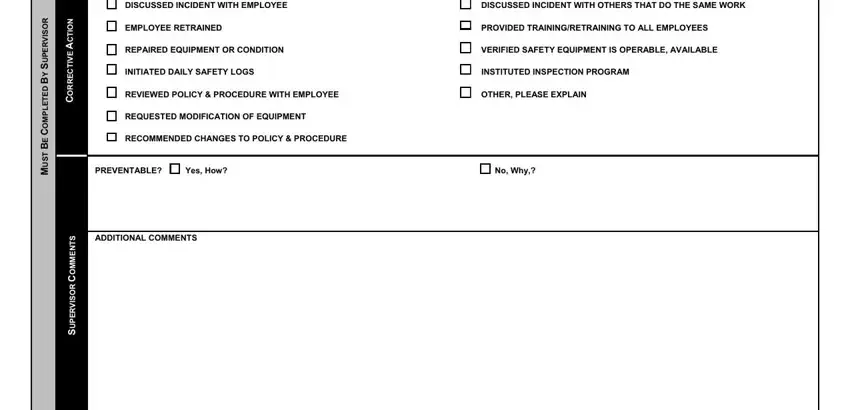
7. Review and Sign the Vehicle Accident Report Form
Ensure all information is accurate, complete, and comprehensive. The employee and a supervisor must sign the form, verifying the correctness of the information. Submit the completed form as directed, typically within 24 hours of the incident, to ensure timely processing.