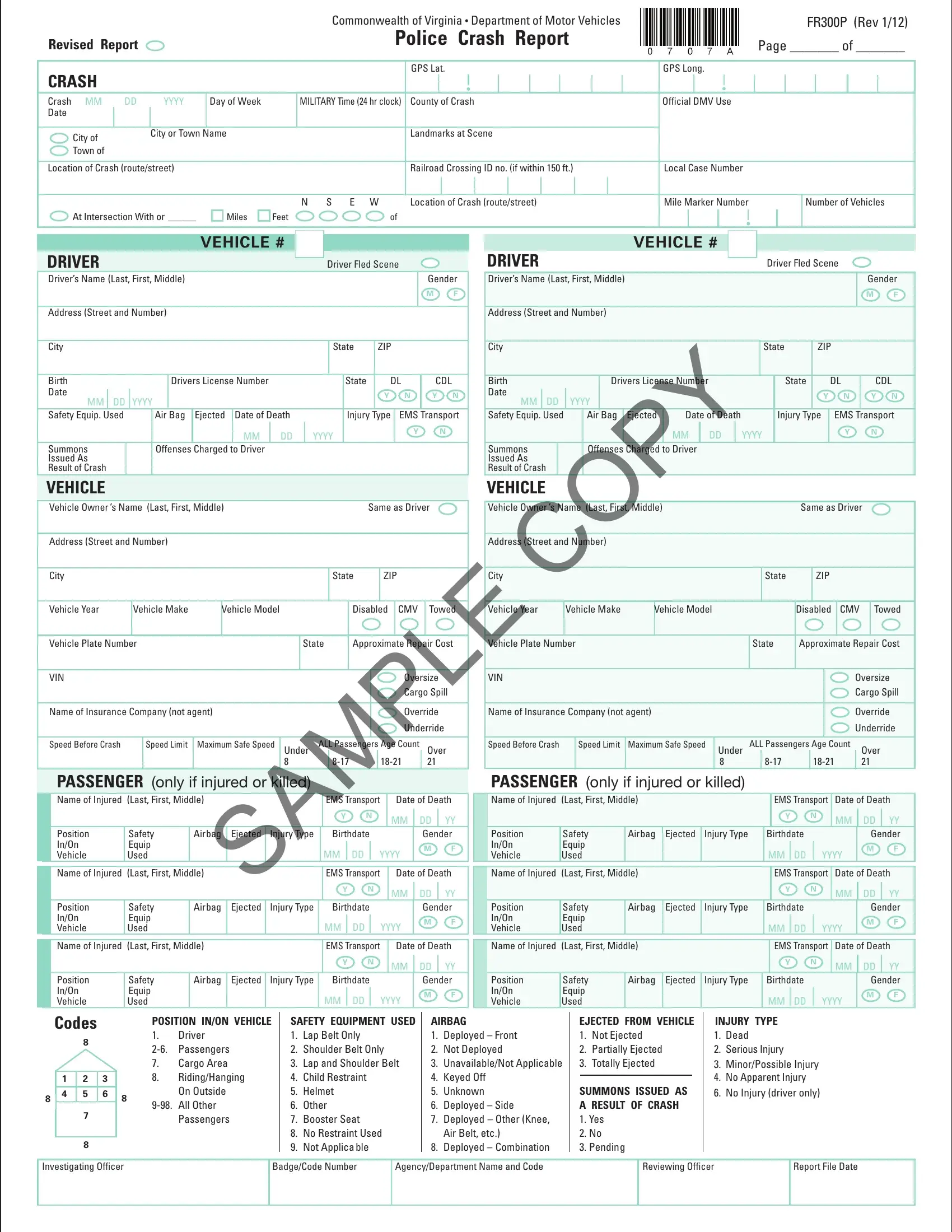
The Commonwealth of Virginia's Department of Motor Vehicles provides the Virginia Police Crash Report Form FR300P as a comprehensive tool for law enforcement officers to document the specifics of vehicular accidents thoroughly. This form captures a wide array of data points, from the basic details of the crash, like date, time, and location, marked by GPS coordinates, to intricate specifics about the involved parties, including drivers, passengers, and vehicles. Characteristics of the crash scene, such as the roadway conditions, weather, and lighting, are systematically recorded alongside a description of the accident, delineating the sequence of events leading to the crash. Moreover, the form addresses commercial vehicle involvement with sections dedicated to cargo details, vehicle configuration, and hazardous material information, if applicable. This structured approach not only facilitates a detailed investigation post-incident but also assists in compiling statistical data to inform future road safety measures. Additionally, the inclusion of diagrams for depicting vehicle positions and movements at the time of the crash offers a visual understanding of the event, further enriching the report's utility in analyses and legal proceedings. Through this form, Virginia aims to streamline accident reporting processes, ensuring accuracy and completeness in capturing crash data.
| Question | Answer |
|---|---|
| Form Name | Virginia Police Crash Report Form |
| Form Length | 6 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 30 sec |
| Other names | fr300 crash report, va fr300 accident report, fr300p, fr300 manual |
