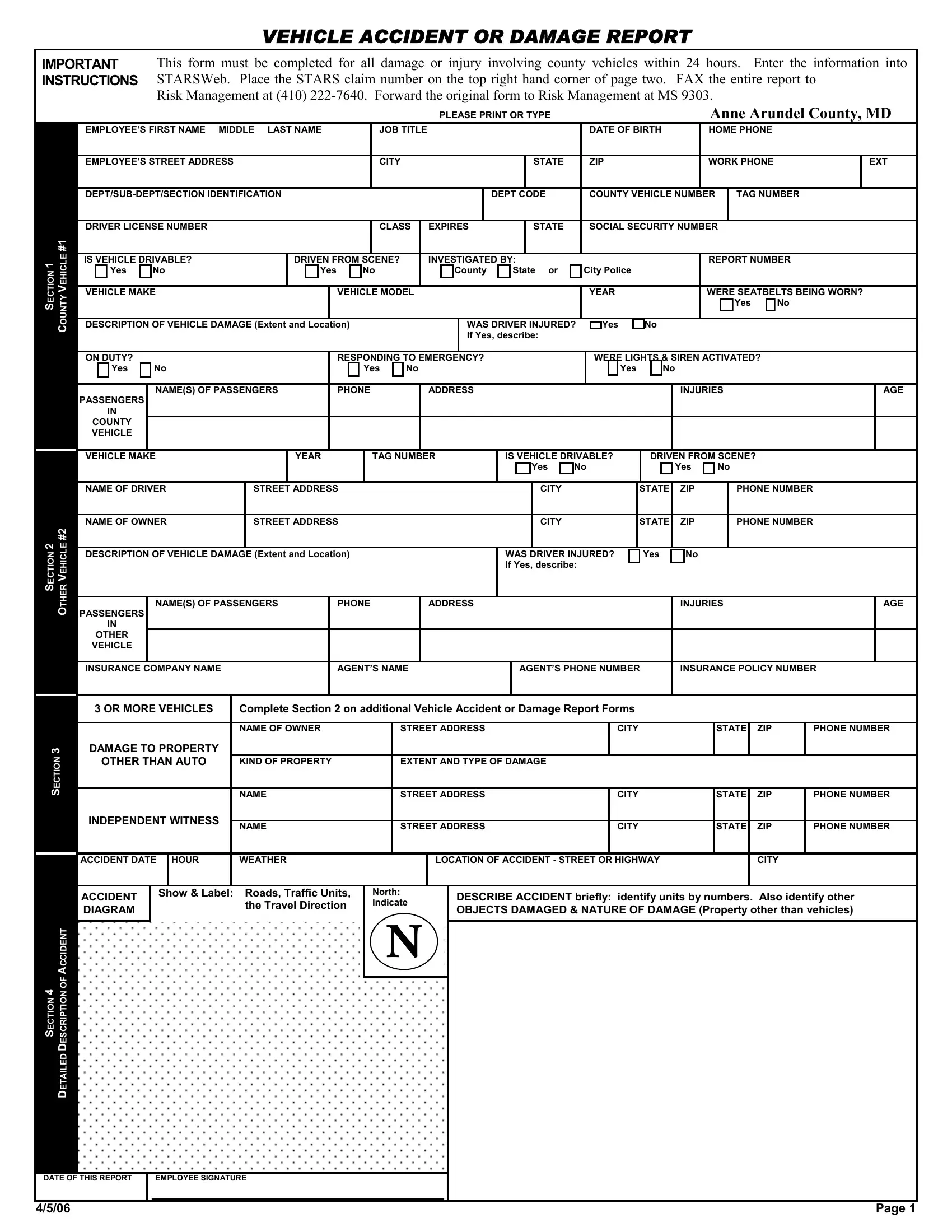
Our printable vehicle accident report form includes personal and car information of the involved parties, specific incident details, and a diagram. It also records the extent of property damage, injuries, witness accounts, and investigative notes from police, if applicable.
Filling out this car accident report form is essential following any incidents involving county vehicles. This way, you document all necessary details for the insurance company, as well as legal and administrative processes. This form must be completed under various conditions:
- Any traffic accident with a county vehicle, irrespective of damage or injuries.
- Incidents resulting in damage to county property or other personal assets.
- Situations where drivers, passengers, or bystanders sustain injuries.
This auto incident report form should be submitted within 24 hours of the incident. Delays or inaccuracies in submission can complicate claims handling or lead to disciplinary actions against drivers involved.
| Question | Answer |
|---|---|
| Form Name | Vehicle Accident Or Damage Report Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 124 |
| Avg. time to fill out | 15 min |
| Other names | vehicle accident investigation report form, car accident report sample PDF, employee vehicle accident report form |