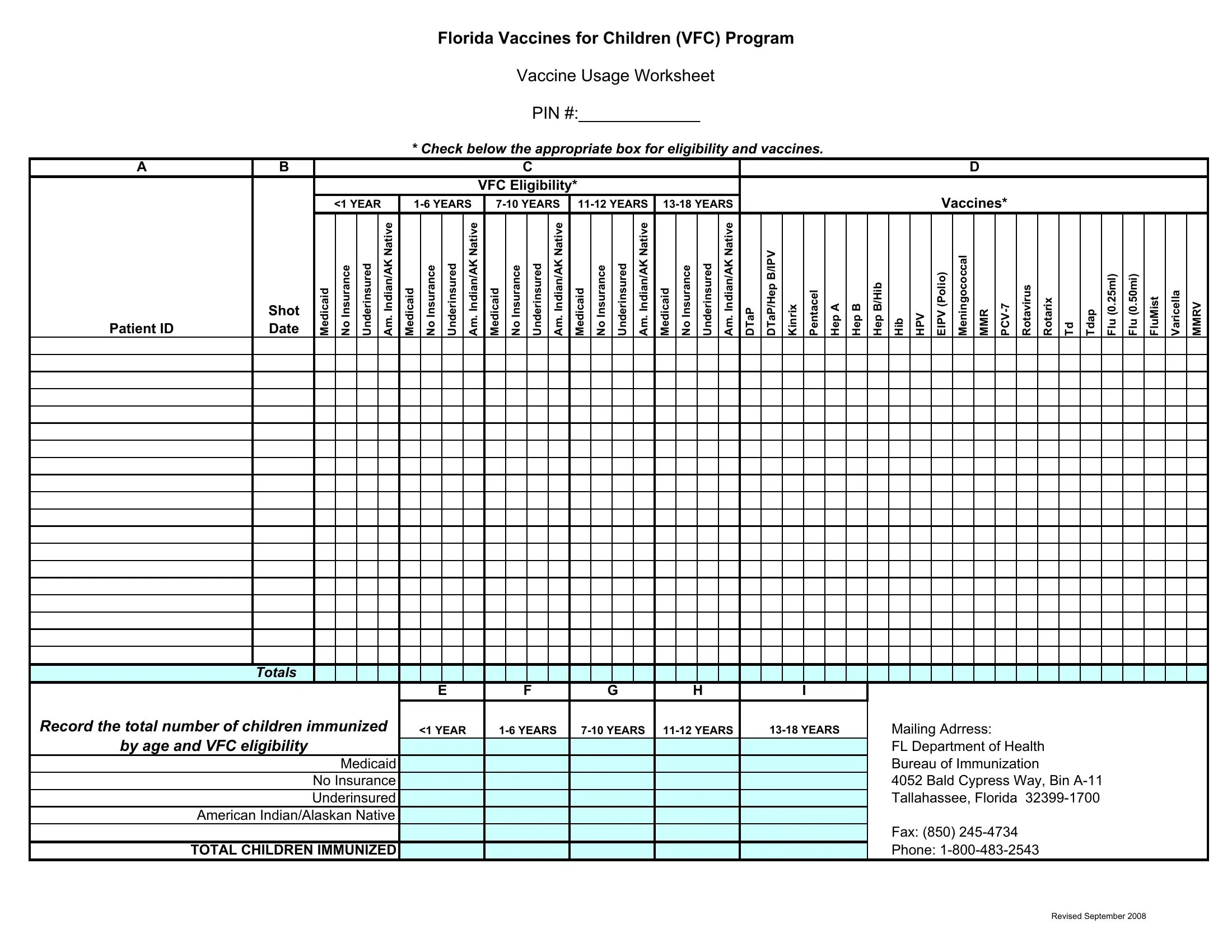
Navigating the landscape of childhood immunizations can be complex, but the Florida Vaccines for Children (VFC) Program Vaccine Usage Worksheet offers a structured approach to ensure all children, regardless of their financial situation, have access to essential vaccinations. This vital tool helps healthcare providers record the immunization status of children according to various factors such as age, VFC eligibility, and the type of vaccine administered. Specifically, the form allows for detailed documentation across different age groups—ranging from babies under one year to adolescents up to 18 years—and categorizes patients based on Medicaid status, lack of insurance, underinsurance, and whether they're of American Indian or Alaskan Native heritage. With sections dedicated to a comprehensive list of vaccines, including DTaP, Hepatitis A and B, HPV, and flu shots among others, the worksheet ensures no child is left behind in their vaccination schedule. Moreover, the form plays a crucial role in public health by facilitating an accurate tally of immunized children, thus aiding the Florida Department of Health's Bureau of Immunization in their efforts to protect all children from vaccine-preventable diseases.
| Question | Answer |
|---|---|
| Form Name | Vfc Vaccine Usage Worksheet Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | florida vaccine for children vaccine usage worksheet, vaccine usage worksheet get, vaccine usage waste worksheet, how to register senior for vaccine in fl |
