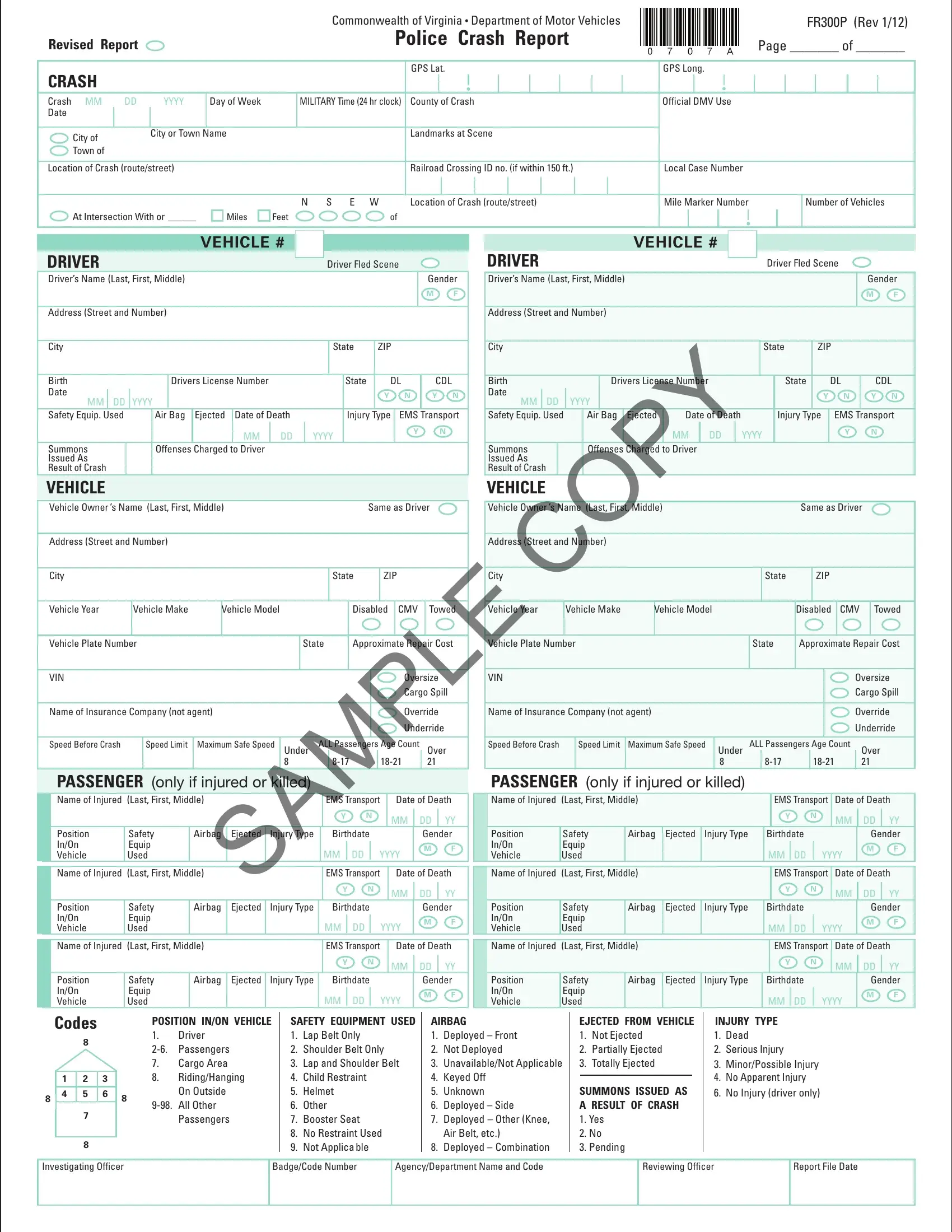
The Commonwealth of Virginia's Department of Motor Vehicles provides the Virginia Police Crash Report Form FR300P as a comprehensive tool for law enforcement officers to document the specifics of vehicular accidents thoroughly. This form captures a wide array of data points, from the basic details of the crash, like date, time, and location, marked by GPS coordinates, to intricate specifics about the involved parties, including drivers, passengers, and vehicles. Characteristics of the crash scene, such as the roadway conditions, weather, and lighting, are systematically recorded alongside a description of the accident, delineating the sequence of events leading to the crash. Moreover, the form addresses commercial vehicle involvement with sections dedicated to cargo details, vehicle configuration, and hazardous material information, if applicable. This structured approach not only facilitates a detailed investigation post-incident but also assists in compiling statistical data to inform future road safety measures. Additionally, the inclusion of diagrams for depicting vehicle positions and movements at the time of the crash offers a visual understanding of the event, further enriching the report's utility in analyses and legal proceedings. Through this form, Virginia aims to streamline accident reporting processes, ensuring accuracy and completeness in capturing crash data.
| Question | Answer |
|---|---|
| Form Name | Virginia Police Crash Report Form |
| Form Length | 6 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 30 sec |
| Other names | fr300 crash report, va fr300 accident report, fr300p, fr300 manual |
|
|
|
|
|
|
|
|
Commonwealth of Virginia • Department of Motor Vehicles |
|
|
|
|
|
|
|
|
|
FR300P (Rev 1/12) |
||||||||||||||||
Revised Report |
|
|
|
|
|
|
Police Crash Report |
|
|
|
|
|
|
Page _______ of _______ |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CRASH |
|
|
|
|
|
|
|
|
GPS Lat. |
GPS Long. |
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Crash MM |
DD |
YYYY |
Day of Week |
|
MILITARY Time (24 hr clock) |
County of Crash |
Official DMV Use |
|
|
|
|
|
|
|
|
|||||||||||||||||||
Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City of |
|
City or Town |
Name |
|
|
Landmarks at Scene |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Town of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Location of Crash (route/street) |
|
|
|
|
|
|
Railroad Crossing ID no. (if within 150 ft.) |
Local Case Number |
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N S E W |
Location of Crash (route/street) |
Mile Marker Number |
|
|
|
|
Number of Vehicles |
|||||||||||||||||||
At Intersection With or ______ |
|
|
Miles |
|
Feet |
of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
DRIVER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Driver Fled Scene |
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
Driver’s Name (Last, First, Middle) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Gender |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Address (Street and Number) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
ZIP |
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Birth |
|
|
|
|
|
Drivers License Number |
|
|
|
|
|
|
|
State |
|
DL |
|
|
CDL |
||||||||||||||||||
|
Date |
|
DD |
|
YYYY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
|
N |
|
|
Y |
N |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
MM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Safety Equip. Used |
|
|
|
|
Air Bag |
Ejected |
|
Date of Death |
|
|
|
Injury |
Type |
|
EMS |
|
Transport |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MM |
|
DD |
|
YYYY |
|
|
|
|
|
|
|
|
Y |
|
|
|
|
N |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Summons |
|
|
|
|
Offenses |
Charged |
to Driver |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Issued As |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Result of Crash |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
VEHICLE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Vehicle Owner ’s Name (Last, First, Middle) |
|
|
|
|
|
|
|
|
|
|
|
|
Same as Driver |
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Address (Street and Number) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
ZIP |
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Vehicle Year |
|
|
Vehicle Make |
|
Vehicle Model |
|
|
|
|
Disabled |
|
CMV |
|
|
Towed |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
Vehicle Plate Number |
|
|
|
|
|
|
|
|
State |
Approximate Repair Cost |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
VIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Oversize |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cargo Spill |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
Name of Insurance Company (not agent) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Override |
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Underride |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
Speed Before Crash |
|
|
|
Speed Limit |
Maximum Safe Speed |
Under |
|
ALL Passengers Age Count |
|
|
Over |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
|
|
21 |
|
|
||||||||
|
|
PASSENGER (only if injured or killed) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
Name of Injured |
(Last, First, Middle) |
|
|
|
|
|
|
|
|
|
EMS Transport |
|
|
|
Date of Death |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
MM |
|
|
DD |
|
YY |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
Position |
Safety |
|
Airbag |
Ejected |
|
Injury Type |
Birthdate |
|
|
|
|
|
|
|
Gender |
|||||||||||||||||||||
|
|
In/On |
Equip |
|
|
|
|
|
|
|
|
|
|
|
|
MM |
|
DD |
|
YYYY |
|
|
|
M |
F |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
Vehicle |
Used |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Injured |
(Last, First, Middle) |
|
|
|
|
|
|
|
|
|
EMS Transport |
|
|
|
Date of Death |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
MM |
|
|
DD |
|
YY |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
Position |
Safety |
|
Airbag |
Ejected |
|
Injury Type |
Birthdate |
|
|
|
|
|
|
|
Gender |
|||||||||||||||||||||
|
|
In/On |
Equip |
|
|
|
|
|
|
|
|
|
|
|
|
MM |
|
DD |
|
YYYY |
|
|
|
M |
F |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
Vehicle |
Used |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Injured |
(Last, First, Middle) |
|
|
|
|
|
|
|
|
|
EMS Transport |
|
|
|
Date of Death |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
|
MM |
|
|
DD |
|
YY |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
Position |
Safety |
|
Airbag |
Ejected |
|
Injury Type |
Birthdate |
|
|
|
|
|
|
|
Gender |
|||||||||||||||||||||
|
|
In/On |
Equip |
|
|
|
|
|
|
|
|
|
|
|
|
MM |
|
DD |
|
YYYY |
|
|
|
M |
F |
|||||||||||||
|
|
Vehicle |
Used |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
VEHICLE # |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
DRIVER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Driver Fled Scene |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Driver’s Name (Last, First, Middle) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Gender |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Address (Street and Number) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
|
|
ZIP |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Birth |
|
|
|
|
Drivers License Number |
|
|
|
State |
|
|
DL |
|
CDL |
||||||||||
|
Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
|
Y |
N |
|
MM |
DD |
YYYY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Safety Equip. Used |
|
Air |
Bag |
Ejected |
Date of Death |
|
|
Injury Type |
|
EMS |
Transport |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
MM |
DD |
|
YYY |
|
|
|
|
|
Y |
|
N |
|
|||
|
Summons |
|
|
|
Offenses |
Charged |
to Driver |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Issued As |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Result of Crash |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vehicle Owner ’s Name (Last, First, Middle) |
|
|
|
|
|
|
|
|
|
Same as Driver |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Address (Street and Number) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
ZIP |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Vehicle Year |
Vehicle Make |
|
Vehicle Model |
|
|
|
|
Disabled |
CMV |
|
Towed |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vehicle Plate Number |
|
|
|
|
|
|
|
|
|
State |
|
Approximate Repair Cost |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Oversize |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cargo Spill |
|||
|
Name of Insurance Company (not agent) |
|
|
|
|
|
|
|
|
|
|
|
|
Override |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Underride |
|||
|
Speed Before Crash |
|
Speed Limit |
Maximum Safe Speed |
Under |
ALL Passengers Age Count |
Over |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
21 |
|
|
||||
|
PASSENGER (only if injured or killed) |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
Name of Injured |
(Last, First, Middle) |
|
|
|
|
|
|
|
EMS Transport |
Date of Death |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
MM |
DD |
YY |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Position |
Safety |
Airbag |
Ejected |
Injury Type |
|
|
Birthdate |
|
|
|
|
Gender |
||||||||||||
|
In/On |
Equip |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
||||
|
Vehicle |
Used |
|
|
|
|
|
|
|
|
|
|
|
MM |
|
DD |
YYYY |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Injured |
(Last, First, Middle) |
|
|
|
|
|
|
|
EMS Transport |
Date of Death |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
MM |
DD |
YY |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Position |
Safety |
Airbag |
Ejected |
Injury Type |
|
|
Birthdate |
|
|
|
|
Gender |
||||||||||||
|
In/On |
Equip |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
||||
|
Vehicle |
Used |
|
|
|
|
|
|
|
|
|
|
|
MM |
|
DD |
YYYY |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Injured |
(Last, First, Middle) |
|
|
|
|
|
|
|
EMS Transport |
Date of Death |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
MM |
DD |
YY |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Position |
Safety |
Airbag |
Ejected |
Injury Type |
|
|
Birthdate |
|
|
|
|
Gender |
||||||||||||
|
In/On |
Equip |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
||||
|
Vehicle |
Used |
|
|
|
|
|
|
|
|
|
|
|
MM |
|
DD |
YYYY |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
Codes
8
|
|
1 |
|
|
2 |
|
|
3 |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
5 |
|
|
6 |
|
|||
8 |
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
||
POSITION IN/ON VEHICLE
1.Driver
7.Cargo Area
8.Riding/Hanging
8On Outside
SAFETY EQUIPMENT USED
1.Lap Belt Only
2.Shoulder Belt Only
3.Lap and Shoulder Belt
4.Child Restraint
5.Helmet
6.Other
7.Booster Seat
8.No Restraint Used
9.Not Applicable
AIRBAG
1.Deployed – Front
2.Not Deployed
3.Unavailable/Not Applicable
4.Keyed Off
5.Unknown
6.Deployed – Side
7.Deployed – Other (Knee, Air Belt, etc.)
8.Deployed – Combination
EJECTED FROM VEHICLE
1.Not Ejected
2.Partially Ejected
3.Totally Ejected
SUMMONS ISSUED AS A RESULT OF CRASH
1.Yes
2.No
3.Pending
INJURY TYPE
1.Dead
2.Serious Injury
3.Minor/Possible Injury
4.No Apparent Injury
6. No Injury (driver only)
Investigating Officer
Badge/Code Number
Agency/Department Name and Code
Reviewing Officer
Report File Date