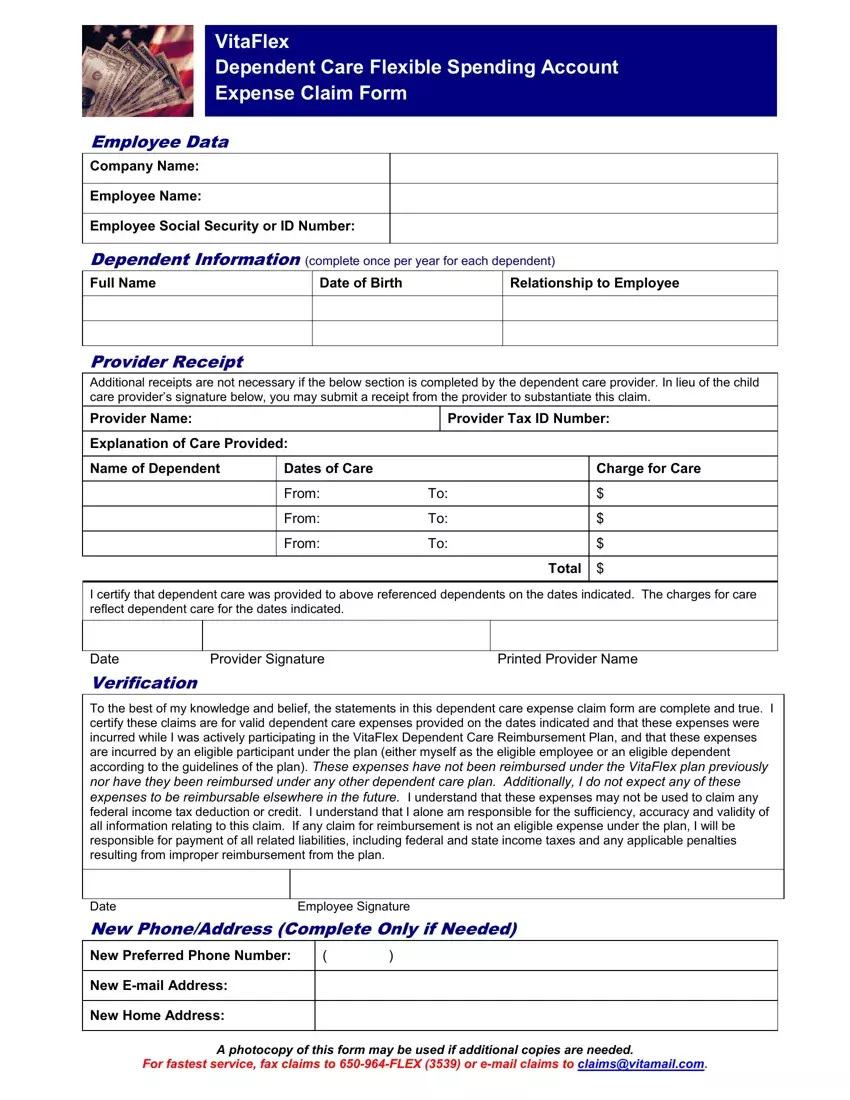
The VitaFlex Dependent Care Flexible Spending Account Expense Claim Form plays a critical role for employees in managing the financial aspects of dependent care. Designed to facilitate the reimbursement for care expenses from the flexible spending account (FSA), this document requires detailed employee data, including company name, employee identification, as well as comprehensive dependent information. Each section of the form meticulously gathers all necessary details such as the full name, date of birth, and relationship of the dependent to the employee, aiming to ensure that all claims are legitimate and within the guidelines set by the plan. The form also emphasizes the importance of provider information, charges for care, and specifically allows for an easy submission process by accepting provider's details and signatures or a receipt in lieu thereof. This substantiation is crucial in certifying that the claimed expenses are for valid dependent care services that were incurred by an eligible participant under the plan. The form includes stern declarations from the employee, asserting that the expenses claimed have not been reimbursed by any other means and acknowledging their responsibility for the accuracy of the submitted information. Such declarations protect against fraudulent claims, safeguarding both the employer's and the employee's interests. Additionally, the form provides sections for updating contact information, ensuring that communication channels remain open and efficient. For expedient processing, it offers multiple submission options, including fax and email, demonstrating a blend of stringent verification processes with user-friendly operational measures.
| Question | Answer |
|---|---|
| Form Name | Vita Flex Fsa Medical Claim Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | vitaclaim dependent flexible spending account, vitaflex login, vita flex login, vita flex medical reimbursement form |
