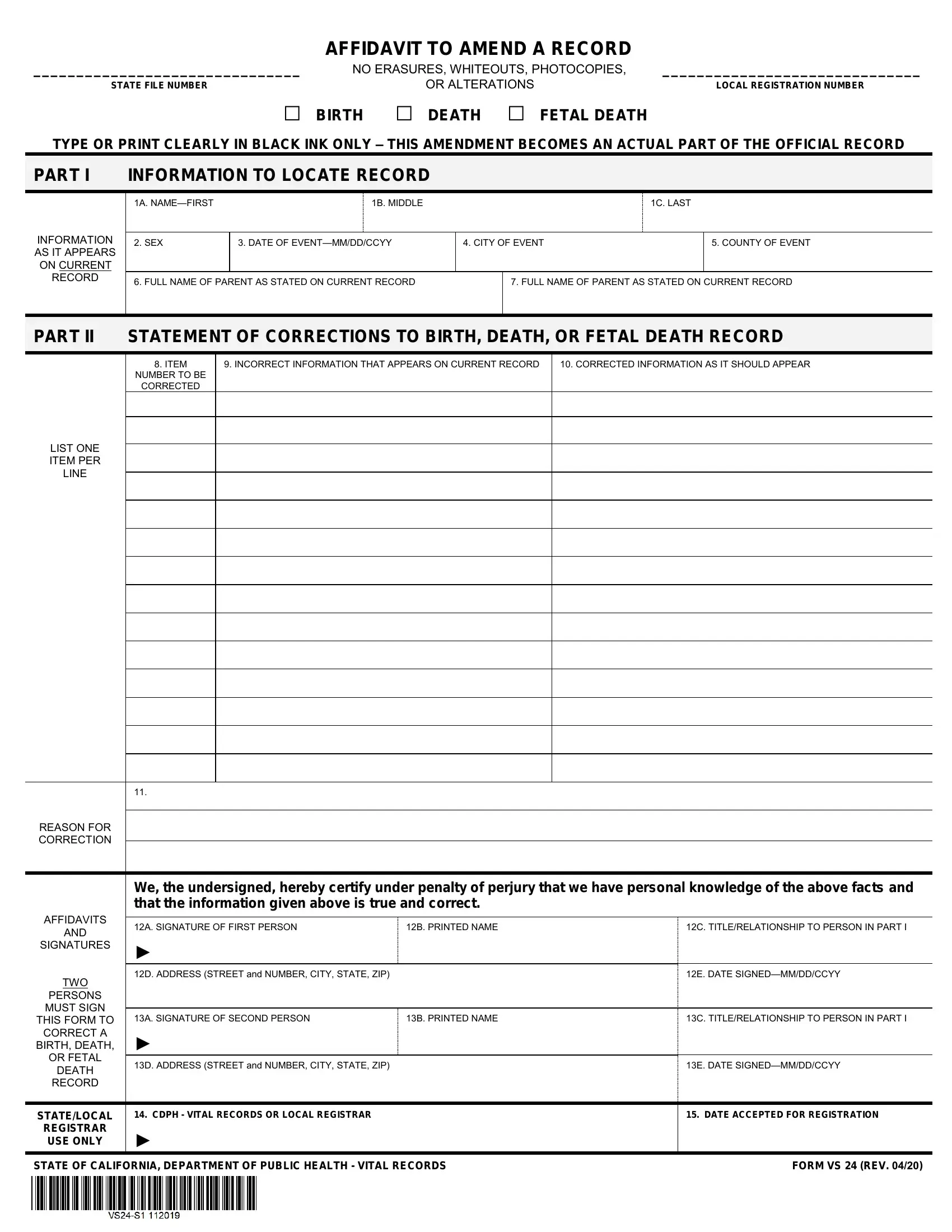
AFFIDAVIT TO AMEND A RECORD
_______________________________ |
NO ERASURES, WHITEOUTS, PHOTOCOPIES, |
______________________________ |
STATE FILE NUMBER |
|
OR ALTERATIONS |
LOCAL REGISTRATION NUMBER |
□ BIRTH |
□ DEATH □ FETAL DEATH |
|
TYPE OR PRINT CLEARLY IN BLACK INK ONLY – THIS AMENDMENT BECOMES AN ACTUAL PART OF THE OFFICIAL RECORD
PART I INFORMATION TO LOCATE RECORD
INFORMATION AS IT APPEARS ON CURRENT RECORD
|
1A. NAME—FIRST |
1B. MIDDLE |
|
|
|
1C. LAST |
|
|
|
|
|
|
|
|
|
2. SEX |
3. DATE OF EVENT—MM/DD/CCYY |
4. CITY OF EVENT |
|
5. COUNTY OF EVENT |
|
|
|
|
|
|
|
|
6. FULL NAME OF PARENT AS STATED ON CURRENT RECORD |
|
|
7. FULL NAME OF PARENT AS STATED ON CURRENT RECORD |
|
|
|
|
|
|
|
|
PART II STATEMENT OF CORRECTIONS TO BIRTH, DEATH, OR FETAL DEATH RECORD
8.ITEM
NUMBER TO BE
CORRECTED
9. INCORRECT INFORMATION THAT APPEARS ON CURRENT RECORD
10. CORRECTED INFORMATION AS IT SHOULD APPEAR
AFFIDAVITS
AND
SIGNATURES
TWO
PERSONS
MUST SIGN
THIS FORM TO
CORRECT A
BIRTH, DEATH,
OR FETAL
DEATH
RECORD
We, the undersigned, hereby certify under penalty of perjury that we have personal knowledge of the above facts and that the information given above is true and correct.
12A. SIGNATURE OF FIRST PERSON12B. PRINTED NAME12C. TITLE/RELATIONSHIP TO PERSON IN PART I
►
12D. ADDRESS (STREET and NUMBER, CITY, STATE, ZIP) |
|
12E. DATE SIGNED—MM/DD/CCYY |
|
|
|
13A. SIGNATURE OF SECOND PERSON |
13B. PRINTED NAME |
13C. TITLE/RELATIONSHIP TO PERSON IN PART I |
► |
|
|
13D. ADDRESS (STREET and NUMBER, CITY, STATE, ZIP) |
|
13E. DATE SIGNED—MM/DD/CCYY |
STATE/LOCAL
REGISTRAR
USE ONLY
14. CDPH - VITAL RECORDS OR LOCAL REGISTRAR
►
15. DATE ACCEPTED FOR REGISTRATION
STATE OF CALIFORNIA, DEPARTMENT OF PUBLIC HEALTH - VITAL RECORDS |
FORM VS 24 (REV. 04/20) |
APPLICATION TO AMEND A RECORD
TYPE OR PRINT CLEARLY IN BLACK INK ONLY
NO ERASURES, WHITEOUTS, PHOTOCOPIES, OR ALTERATIONS
If an acceptable application to amend the record is registered within one year of the date of the event, there is no processing fee; however, there is a fee required for a certified copy.
Enclosed is the fee of $___________________________ for a certified copy of the newly amended record.
If an acceptable application to amend the record is registered one year or more after the date of the event, there is a fee for filing the affidavit, which includes one certified copy. There is a fee for each additional certified copy. Please contact your Local Registrar, County Recorder, or the State Registrar for the current fees, or visit our website at www.cdph.ca.gov.
Enclosed is the fee of $___________________________ for filing the affidavit and one certified copy of the newly amended record.
Enclosed is the fee of $___________________________ for an additional certified copy(ies) of the newly amended record.
______________________________________________ |
______________________________________________________________________ |
Printed Name of Applicant |
|
Mailing Address of Applicant |
Telephone Number ( |
) ________________________ |
______________________________________________________________________ |
Email Address: _________________________________ |
City, State, ZIP Code |
|
GENERAL INFORMATION
1.The original certificate cannot be altered.
2.This amendment becomes a part of the original record, so please type or print clearly in black ink only.
3.Please submit original amendment form only. Photocopies of the amendment form will be rejected.
4.Your certified copy will include a copy of the original certificate with a copy of the amendment.
5.The certified copy of the certificate and the attached amendment must remain together for the certified copy to be valid.
READ INSTRUCTIONS CAREFULLY BEFORE COMPLETING THE FORM
1.A Notarized Sworn Statement is required when requesting a certified authorized copy of the amended certificate. For more information please visit our website at www.cdph.ca.gov.
2.This form becomes a part of the original record – type or print clearly in black ink only.
3.No erasures, whiteouts, photocopies, or alterations allowed.
4.Complete Part I, Items 1 – 7, with the information as it appears on the current certificate.
5.Enter the certificate item number(s) to be corrected, either from the original or subsequent amendment, in Part II—Item 8. List one item per line.
6.Enter the incorrect information that appears on the current certificate in the line(s) provided below Item 9.
7.In Item 10, enter the correct information as it should appear for each item listed in Item 9.
8.Enter the reason for the correction in Item 11.
9.Read the affidavit statement. Two persons who are certifying to the statement of corrections must sign the form.
10.Do not write in Items 14 or 15. This space is reserved for State or Local Registrar use only.
11.Make check or money order payable to CDPH - Vital Records. When the paperwork is properly completed and signed by two parties, return this form, together with the required fee(s), to:
California Department of Public Health
Vital Records - Amendments - MS 5105
P.O. Box 997410
Sacramento, CA 95899-7410