
In case you wish to fill out agreement section 32 form, it's not necessary to download and install any kind of software - just use our online PDF editor. FormsPal expert team is constantly endeavoring to improve the tool and help it become much better for clients with its handy features. Bring your experience to the next level with continuously developing and fantastic opportunities we provide! All it requires is a few easy steps:
Step 1: Access the PDF inside our tool by pressing the "Get Form Button" in the top section of this page.
Step 2: Using our online PDF file editor, it is possible to do more than merely fill in blank fields. Try all of the functions and make your forms appear professional with custom textual content added in, or adjust the original input to perfection - all that supported by an ability to insert any graphics and sign it off.
As for the fields of this specific form, here's what you should know:
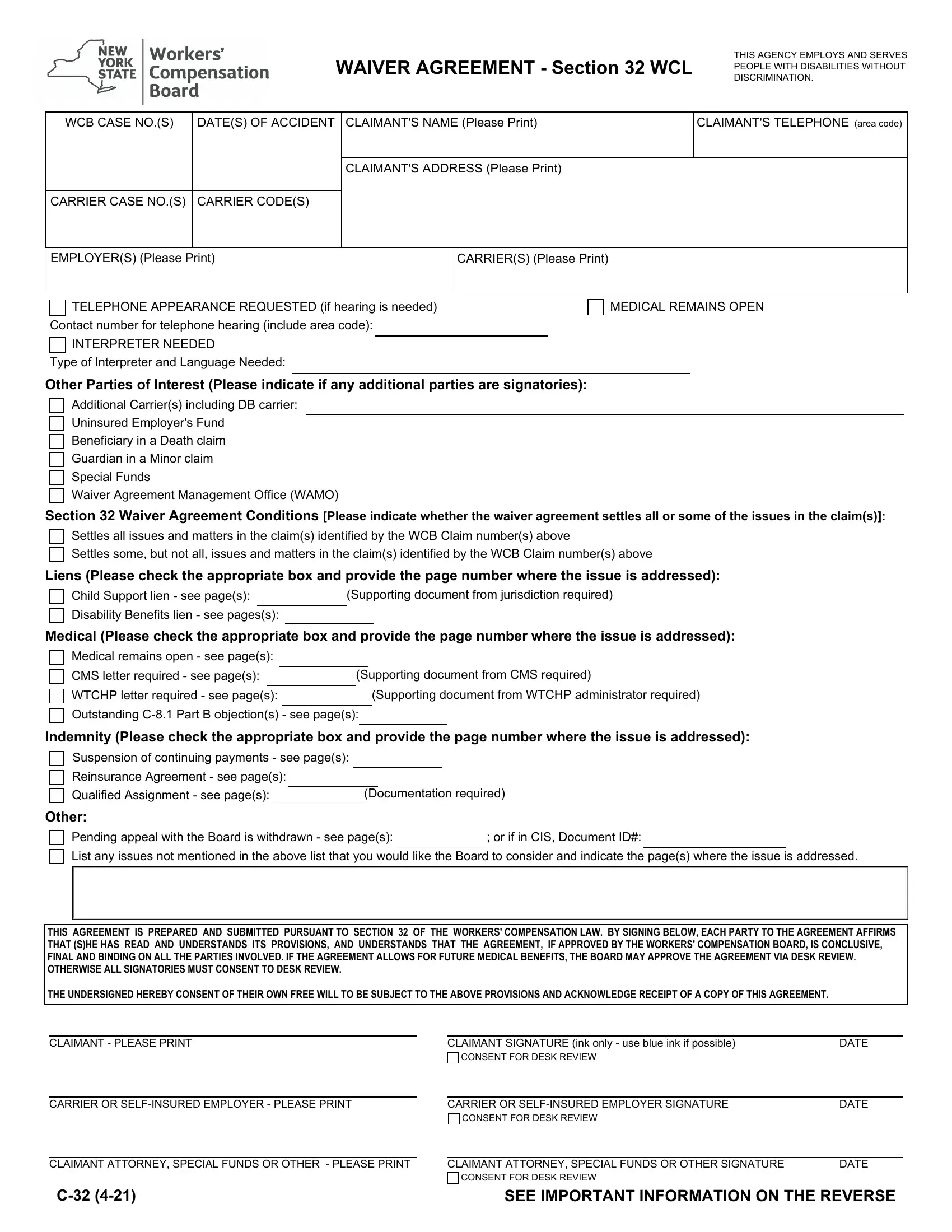
1. To start with, once filling out the agreement section 32 form, begin with the form section that has the subsequent fields:
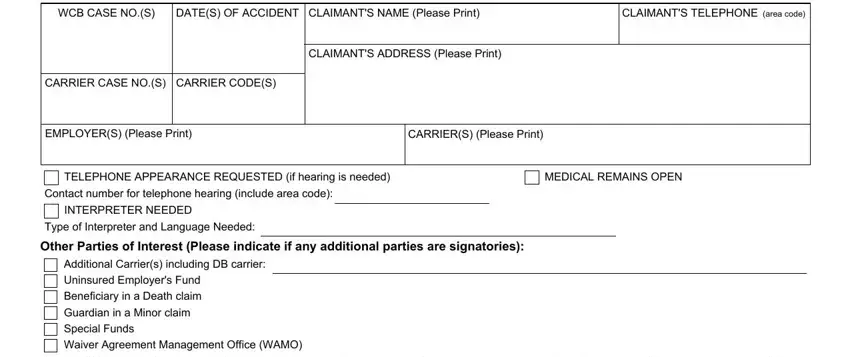
2. The subsequent part is to fill in these particular blank fields: Section Waiver Agreement, Settles all issues and matters in, Settles some but not all issues, Liens Please check the appropriate, Child Support lien see pages, Supporting document from, Disability Benefits lien see, Medical Please check the, Medical remains open see pages, CMS letter required see pages, Supporting document from CMS, WTCHP letter required see pages, Supporting document from WTCHP, Outstanding C Part B objections, and Indemnity Please check the.
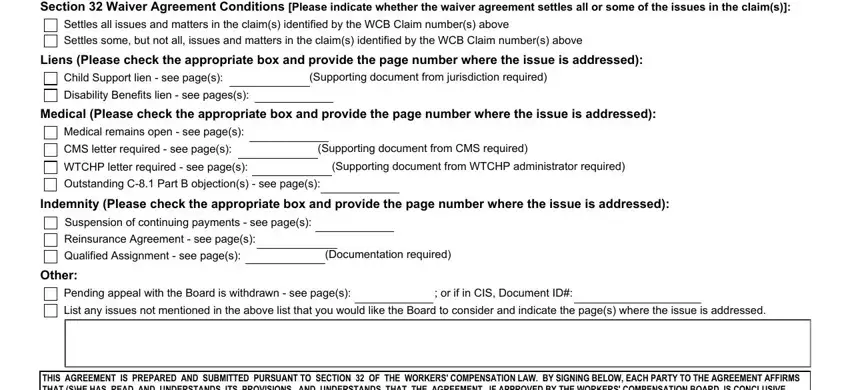
3. This 3rd part should be relatively simple, THIS AGREEMENT IS PREPARED AND, CLAIMANT PLEASE PRINT, CLAIMANT SIGNATURE ink only use, CONSENT FOR DESK REVIEW, CARRIER OR SELFINSURED EMPLOYER, CARRIER OR SELFINSURED EMPLOYER, CONSENT FOR DESK REVIEW, DATE, DATE, CLAIMANT ATTORNEY SPECIAL FUNDS OR, CLAIMANT ATTORNEY SPECIAL FUNDS OR, DATE, CONSENT FOR DESK REVIEW, and SEE IMPORTANT INFORMATION ON THE - all these empty fields has to be completed here.
It is easy to make a mistake when filling out your CONSENT FOR DESK REVIEW, so be sure to reread it prior to deciding to submit it.
Step 3: Make certain the information is right and then click on "Done" to proceed further. Join us right now and immediately get access to agreement section 32 form, prepared for download. Every edit you make is handily saved , which means you can change the file at a later time as required. FormsPal ensures your information privacy via a secure method that never saves or distributes any kind of sensitive information provided. Be confident knowing your paperwork are kept safe each time you use our editor!