

Using PDF documents online is certainly very simple using our PDF editor. Anyone can fill out wage and salary verification form here without trouble. FormsPal professional team is continuously endeavoring to improve the editor and ensure it is even better for clients with its handy functions. Bring your experience to a higher level with continually growing and unique possibilities we provide! To get the ball rolling, take these easy steps:
Step 1: Press the "Get Form" button above. It is going to open our pdf editor so you can begin filling out your form.
Step 2: Using our online PDF editor, you can actually accomplish more than simply complete blank fields. Express yourself and make your documents seem high-quality with custom textual content added, or modify the original input to excellence - all that comes along with the capability to add any photos and sign the document off.
It will be simple to complete the form using this detailed guide! Here is what you should do:
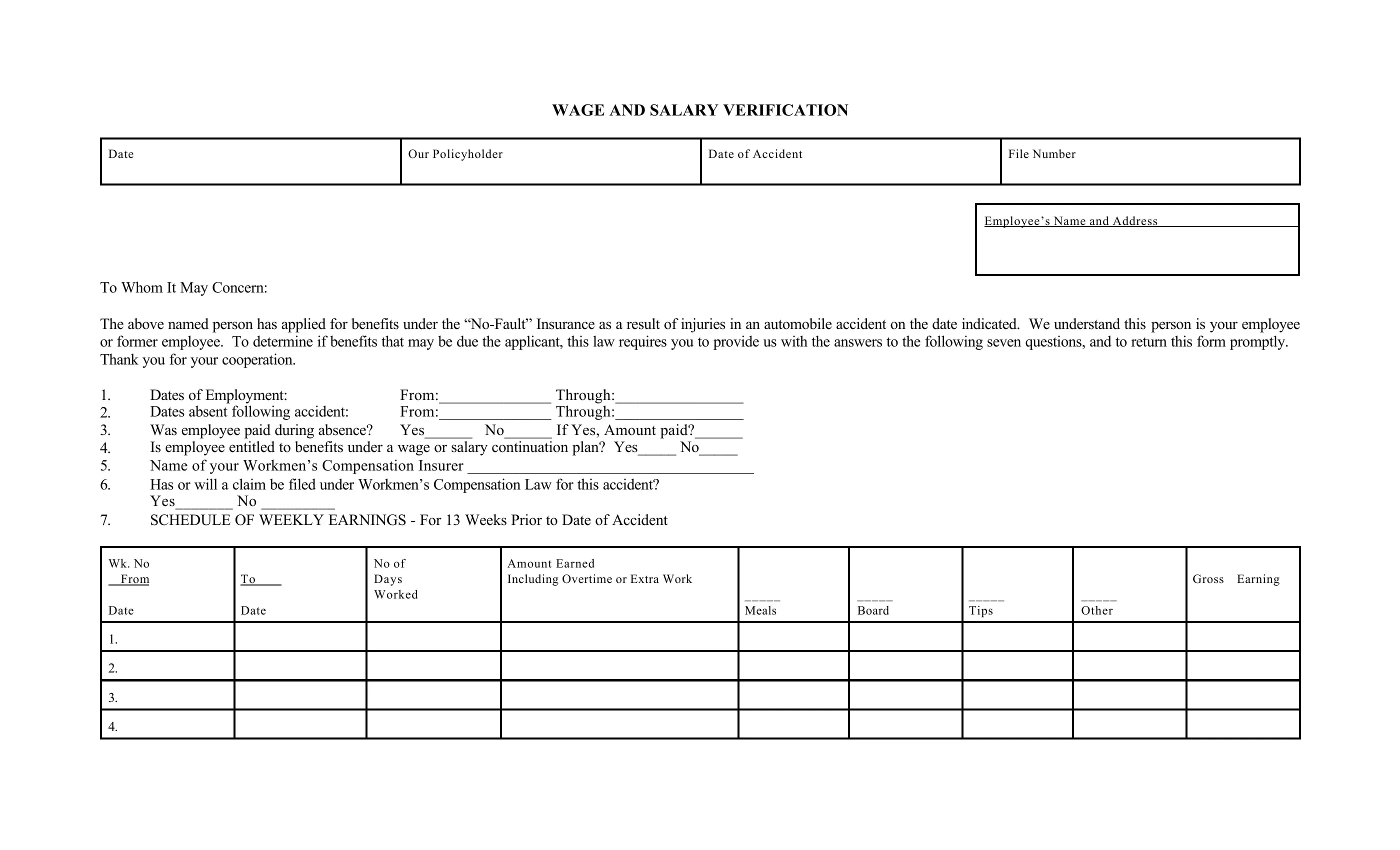
1. When completing the wage and salary verification form, make certain to include all necessary blank fields within its relevant area. It will help to facilitate the process, allowing your details to be processed swiftly and correctly.
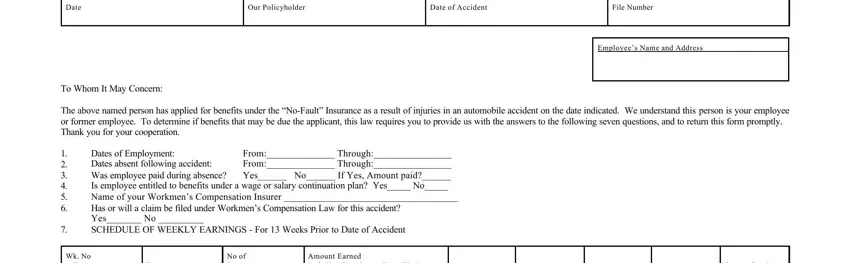
2. The next step is usually to complete these blanks: Date, Meals, Board, Tips, Other, and Wk No From Date.

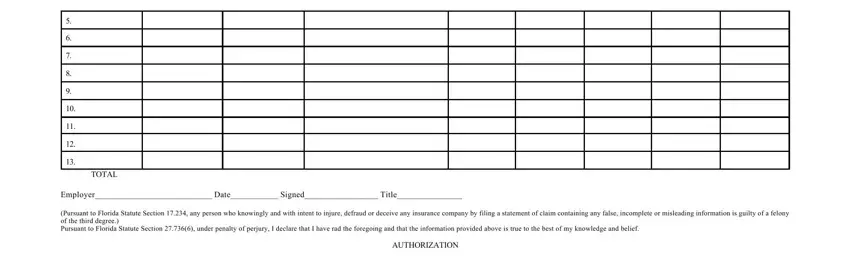
3. This next segment is all about TOTAL, Employer Date Signed Title, Pursuant to Florida Statute, and AUTHORIZATION - complete each of these blank fields.
4. Filling in I the undersigned client hereby, and EMPLOYEECLIENT is essential in this stage - be sure to be patient and be attentive with every single empty field!
Always be very mindful when filling in EMPLOYEECLIENT and I the undersigned client hereby, since this is where most people make some mistakes.
Step 3: Before moving on, ensure that all blanks have been filled out the right way. When you think it is all fine, press “Done." Create a 7-day free trial subscription at FormsPal and acquire immediate access to wage and salary verification form - with all changes preserved and accessible from your FormsPal account page. When using FormsPal, you'll be able to fill out forms without being concerned about data incidents or entries being shared. Our protected software helps to ensure that your personal details are kept safely.