You can certainly complete documents through our PDF editor. Editing the officers exclusion form for texas file is effortless in case you try out the next steps:
Step 1: To get going, select the orange button "Get Form Now".
Step 2: Now it's easy to manage your officers exclusion form for texas. This multifunctional toolbar allows you to include, remove, transform, and highlight text or perform other sorts of commands.
Enter the requested details in every single part to create the PDF officers exclusion form for texas
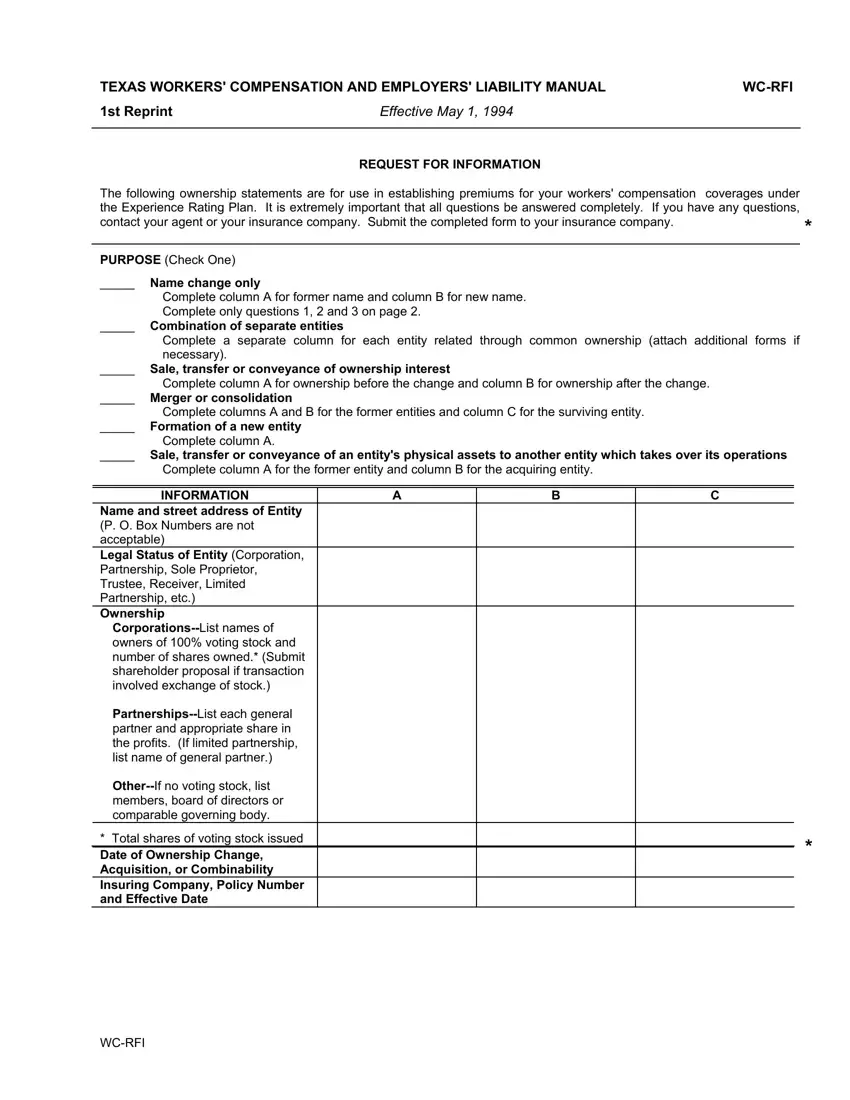
Inside the segment INFORMATION Name and street, owners of voting stock and number, PartnershipsList each general, OtherIf no voting stock list, members board of directors or, and Total shares of voting stock type in the information that the application asks you to do.
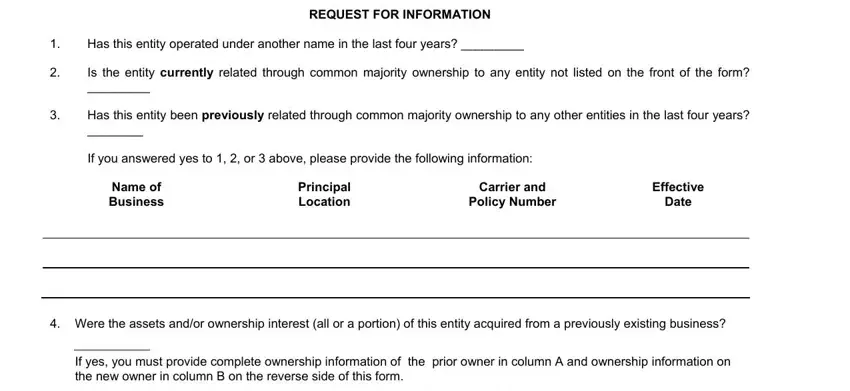
Within the section dealing with Has this entity operated under, REQUEST FOR INFORMATION, Is the entity currently related, Has this entity been previously, If you answered yes to or above, Name of Business, Principal Location, Carrier and Policy Number, Effective Date, Were the assets andor ownership, and If yes you must provide complete, it's important to put down some significant data.
The If this is a partial sale transfer, a Explain what portion or location, b Was this entity insured under a, If not specify the, entities with which it was combined, c What entities will the seller, This is to certify that the, Name of insured, Name of person completing form, Signature of Owner Partner or, Title, Print name of above signature, and Date field enables you to specify the rights and obligations of both sides.
Step 3: Choose the Done button to ensure that your finalized document could be transferred to any electronic device you select or forwarded to an email you indicate.
Step 4: You could make copies of the form tostay clear of all forthcoming concerns. Don't be concerned, we don't disclose or record your data.
