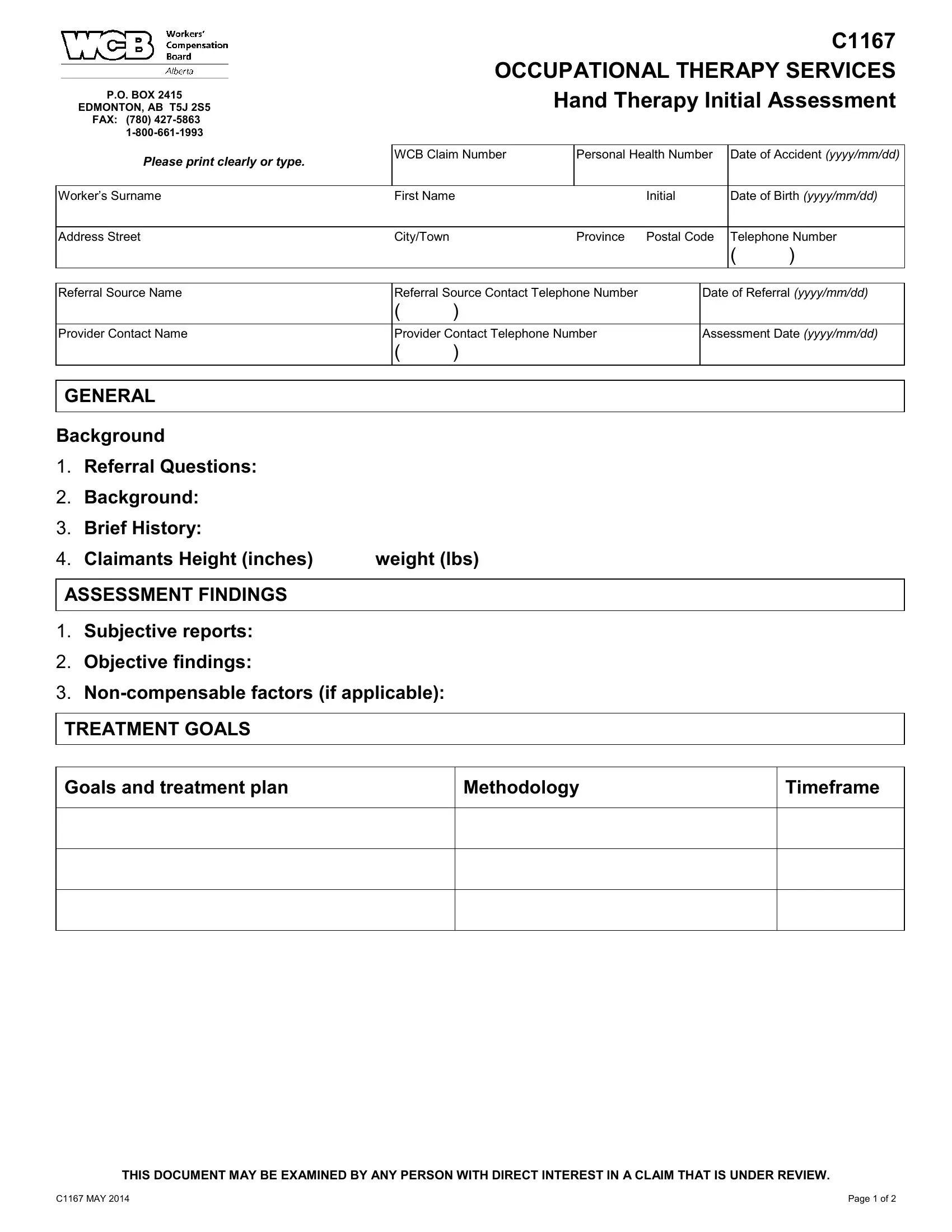
Dealing with injuries at work can lead to a complex recovery process involving many steps and documentation. One such vital piece of documentation is the Worker's Compensation Board (WCB) C1167 form, specifically designed for occupational therapy services focusing on hand therapy initial assessments. This form is required to accurately capture and communicate the essential details about an injured worker’s condition and the proposed treatment plan, making it a cornerstone in the path to rehabilitation. It is meticulously structured to include information about the affected worker such as their WCB claim number, personal health number, and the specifics of the accident. It also gathers comprehensive data about the referring source and the provider performing the assessment. Additionally, the form delves into the particulars of the injury, outlining the worker’s subjective reports, objective findings, and non-compensable factors if present. It sets forth the goals for the treatment and offers an outline for the planned approach, including methodology and anticipated timeframes for recovery. The form even addresses the worker's capability for modified or alternative duties, contributing to a holistic overview of their current situation and the path forward. By filling out this form with clear and precise information, it lays the groundwork for an effective and efficient recovery process, ensuring that all parties have a mutual understanding of the case at hand.
| Question | Answer |
|---|---|
| Form Name | Wcb Form C1167 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | moca version 8 3 instructions, mental status checklist for adults, occupational therapy ergonomic assessment ontario, occupational therapy initial interview template |
P.O. BOX 2415
EDMONTON, AB T5J 2S5 FAX: (780)
C1167 OCCUPATIONAL THERAPY SERVICES Hand Therapy Initial Assessment
Please print clearly or type. |
WCB Claim Number |
Personal Health Number |
Date of Accident (yyyy/mm/dd) |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Worker’s Surname |
First Name |
|
Initial |
Date of Birth (yyyy/mm/dd) |
|||
|
|
|
|
|
|
|
|
Address Street |
City/Town |
|
Province |
Postal Code |
Telephone Number |
||
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|||
|
|
|
|
||||
Referral Source Name |
Referral Source Contact Telephone Number |
|
Date of Referral (yyyy/mm/dd) |
||||
|
( |
) |
|
|
|
|
|
|
|
|
|
||||
Provider Contact Name |
Provider Contact Telephone Number |
|
Assessment Date (yyyy/mm/dd) |
||||
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
GENERAL
Background
1.Referral Questions:
2.Background:
3.Brief History:
4. Claimants Height (inches) |
weight (lbs) |
ASSESSMENT FINDINGS
1.Subjective reports:
2.Objective findings:
3.
TREATMENT GOALS
Goals and treatment plan
Methodology
Timeframe
THIS DOCUMENT MAY BE EXAMINED BY ANY PERSON WITH DIRECT INTEREST IN A CLAIM THAT IS UNDER REVIEW.
C1167 MAY 2014 |
Page 1 of 2 |

OTHER
Can the worker perform modified or alternative duties?
Yes
No
If, yes – please specify work capability:
Sedentary |
Light |
Medium |
Heavy
Are there any specific tasks that should be avoided?:
Are there any other factors that are affecting recovery?:
If you have any questions regarding the information or would like to discuss, please contact the undersigned.
|
( |
) |
|
|
|
Provider's Name |
|
Telephone Number |
|
Date (yyyy/mm/dd) |
|
THIS DOCUMENT MAY BE EXAMINED BY ANY PERSON WITH DIRECT INTEREST IN A CLAIM THAT IS UNDER REVIEW.
C1167 MAY 2014 |
Page 2 of 2 |