Are you a worker in Ontario and have recently been injured or become ill on the job? Understanding accident benefits and how to get financial assistance promptly can be overwhelming, especially if this is your first time dealing with it. Fortunately, WSIB (Workplace Safety & Insurance Board) has launched the C1167 form - an easy-to-follow patient handbook which provides workers like yourself with everything you need to know about submitting for financial aid through materials such as health management forms, appeal forms, advice letters and more. In this blog post, we’ll give you an overview of what WCB Form C1167 is all about including step by step instructions on how to fill out and submit the form.
| Question | Answer |
|---|---|
| Form Name | Wcb Form C1167 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | moca version 8 3 instructions, mental status checklist for adults, occupational therapy ergonomic assessment ontario, occupational therapy initial interview template |
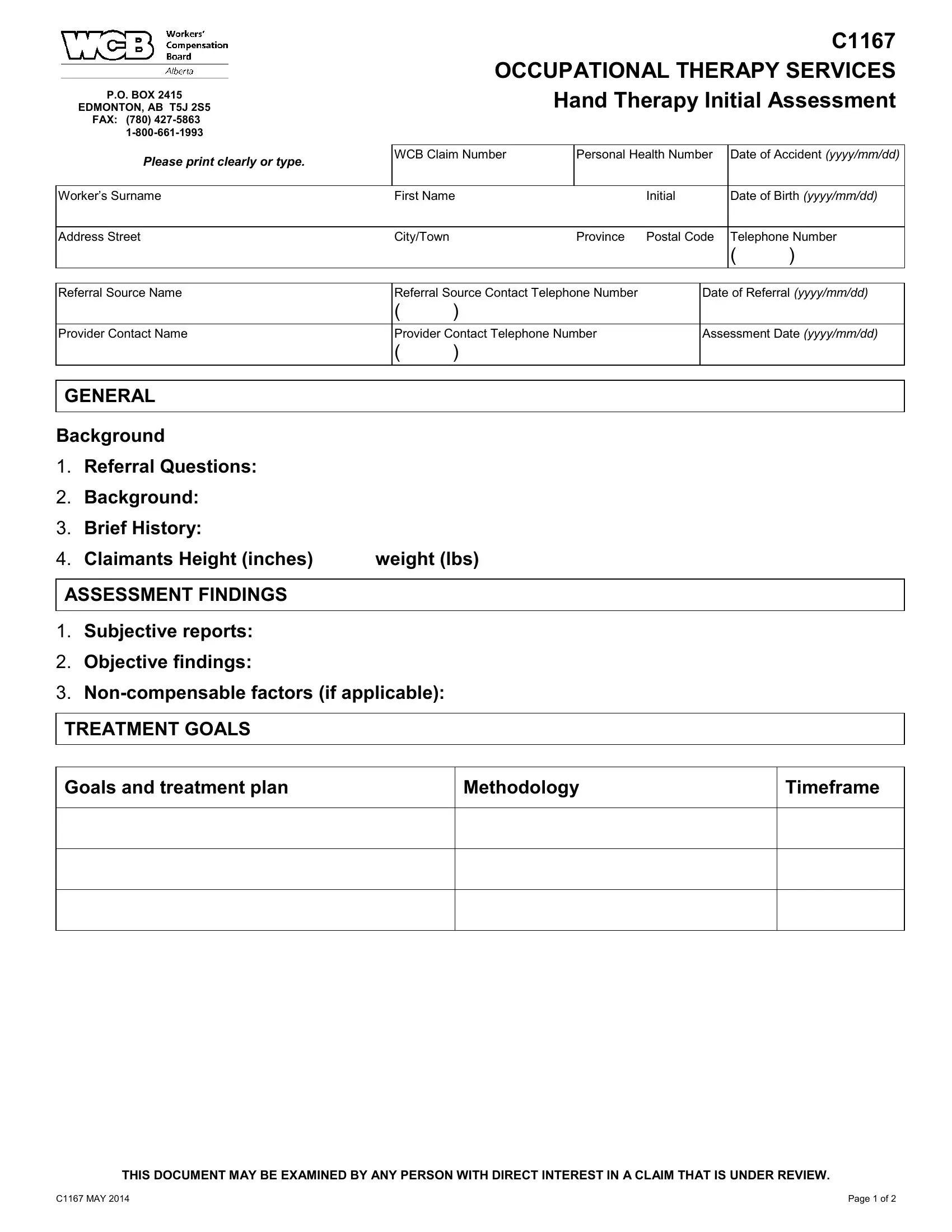
P.O. BOX 2415
EDMONTON, AB T5J 2S5 FAX: (780)
C1167 OCCUPATIONAL THERAPY SERVICES Hand Therapy Initial Assessment
Please print clearly or type. |
WCB Claim Number |
Personal Health Number |
Date of Accident (yyyy/mm/dd) |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Worker’s Surname |
First Name |
|
Initial |
Date of Birth (yyyy/mm/dd) |
|||
|
|
|
|
|
|
|
|
Address Street |
City/Town |
|
Province |
Postal Code |
Telephone Number |
||
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|||
|
|
|
|
||||
Referral Source Name |
Referral Source Contact Telephone Number |
|
Date of Referral (yyyy/mm/dd) |
||||
|
( |
) |
|
|
|
|
|
|
|
|
|
||||
Provider Contact Name |
Provider Contact Telephone Number |
|
Assessment Date (yyyy/mm/dd) |
||||
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
GENERAL
Background
1.Referral Questions:
2.Background:
3.Brief History:
4. Claimants Height (inches) |
weight (lbs) |
ASSESSMENT FINDINGS
1.Subjective reports:
2.Objective findings:
3.
TREATMENT GOALS
Goals and treatment plan
Methodology
Timeframe
THIS DOCUMENT MAY BE EXAMINED BY ANY PERSON WITH DIRECT INTEREST IN A CLAIM THAT IS UNDER REVIEW.
C1167 MAY 2014 |
Page 1 of 2 |

OTHER
Can the worker perform modified or alternative duties?
Yes
No
If, yes – please specify work capability:
Sedentary |
Light |
Medium |
Heavy
Are there any specific tasks that should be avoided?:
Are there any other factors that are affecting recovery?:
If you have any questions regarding the information or would like to discuss, please contact the undersigned.
|
( |
) |
|
|
|
Provider's Name |
|
Telephone Number |
|
Date (yyyy/mm/dd) |
|
THIS DOCUMENT MAY BE EXAMINED BY ANY PERSON WITH DIRECT INTEREST IN A CLAIM THAT IS UNDER REVIEW.
C1167 MAY 2014 |
Page 2 of 2 |