
WCC can be completed online in no time. Simply try FormsPal PDF editor to accomplish the job promptly. In order to make our tool better and more convenient to use, we consistently work on new features, taking into consideration feedback coming from our users. Getting underway is simple! All you have to do is follow the following easy steps below:
Step 1: Simply click the "Get Form Button" in the top section of this page to access our pdf editing tool. There you will find everything that is necessary to work with your document.
Step 2: The tool enables you to change PDF documents in many different ways. Enhance it by adding your own text, correct what's originally in the file, and include a signature - all at your disposal!
As for the blank fields of this precise PDF, this is what you should know:
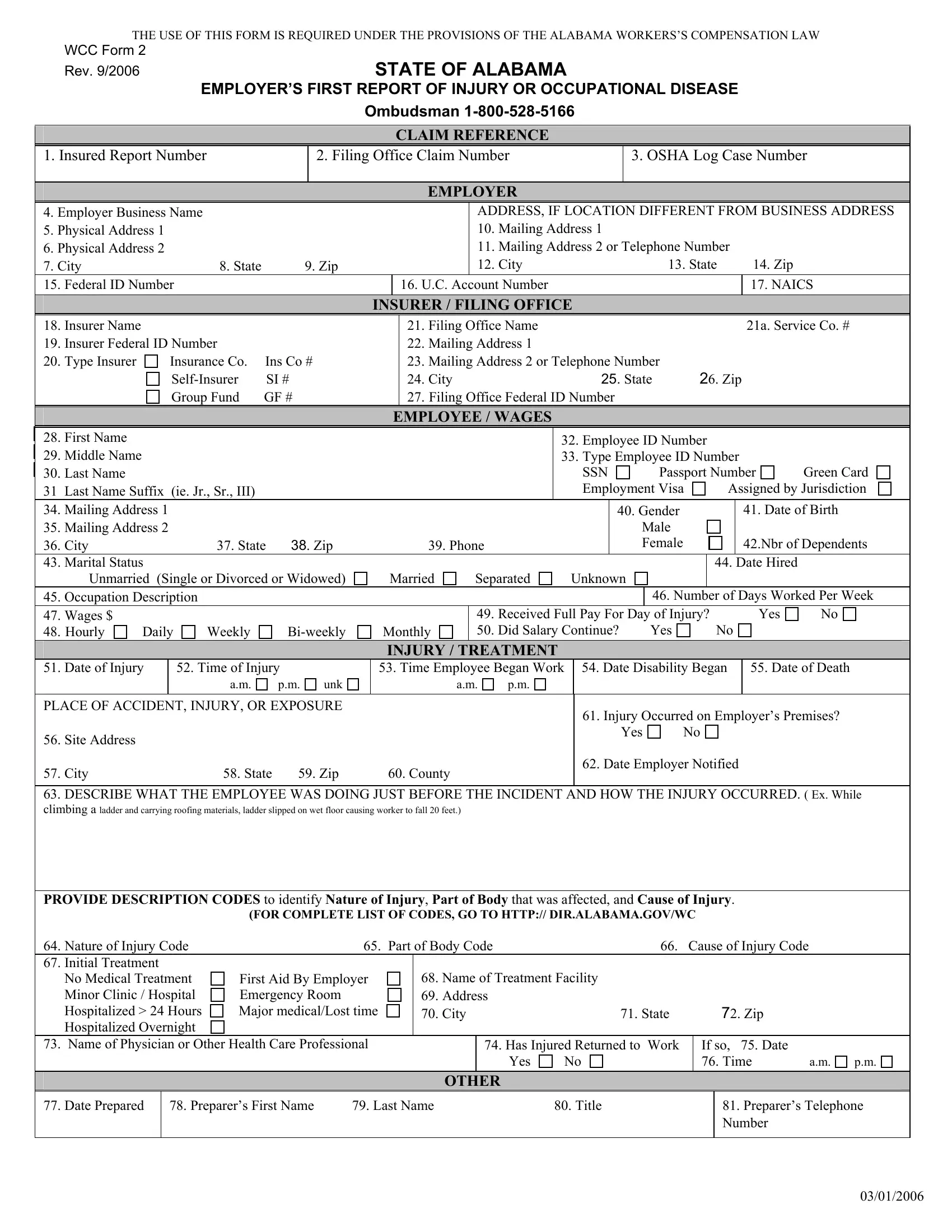
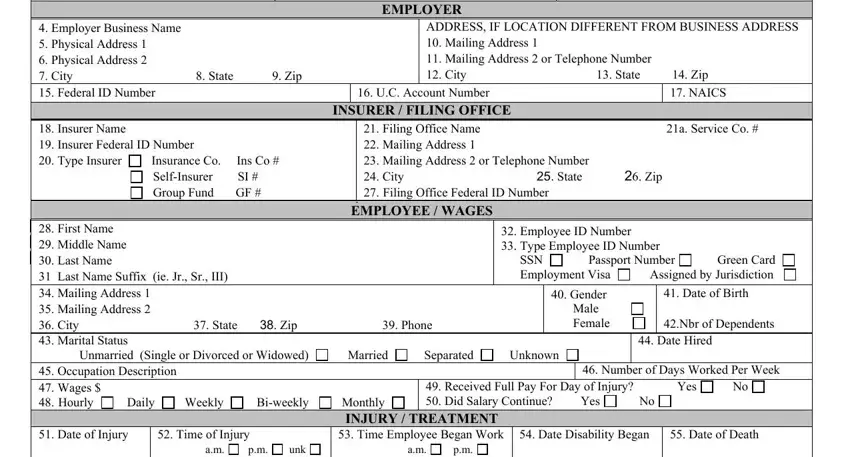
1. To start with, when filling in the WCC, start with the page that features the following fields:
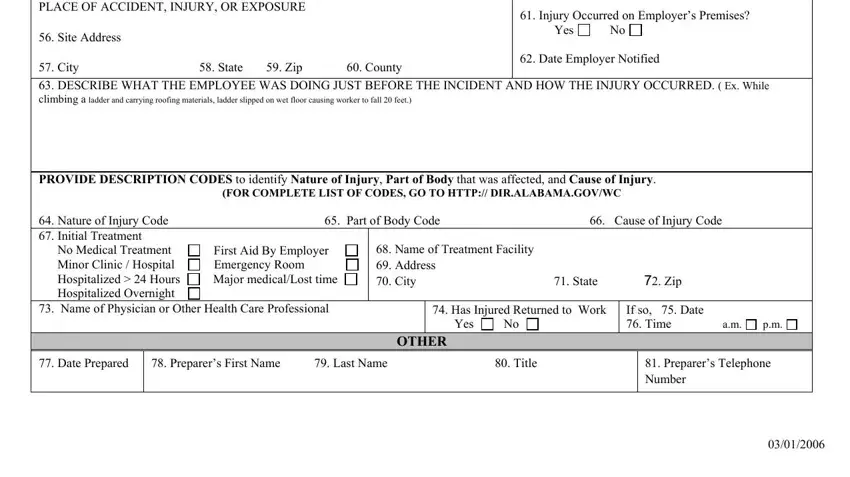
2. Given that the previous section is done, you're ready add the essential details in PLACE OF ACCIDENT INJURY OR, Injury Occurred on Employers, PROVIDE DESCRIPTION CODES to, FOR COMPLETE LIST OF CODES GO TO, Nature of Injury Code Part of, Name of Treatment Facility, First Aid By Employer Emergency, Has Injured Returned to Work Yes, If so Date Time am, Date Prepared, Preparers First Name Last Name, Preparers Telephone Number, and OTHER so you're able to progress to the next step.
People generally make errors while filling out Nature of Injury Code Part of in this area. Don't forget to reread everything you type in right here.
Step 3: Prior to submitting your document, you should make sure that blank fields were filled out the right way. Once you believe it's all good, click “Done." Create a 7-day free trial option with us and gain direct access to WCC - with all transformations saved and available inside your personal cabinet. We do not share the details you use while working with forms at our website.