

Using the online PDF editor by FormsPal, you can easily complete or modify hospitalist here. To make our editor better and more convenient to use, we constantly design new features, with our users' suggestions in mind. To get the ball rolling, consider these easy steps:
Step 1: Simply click the "Get Form Button" above on this page to start up our form editing tool. Here you'll find all that is needed to work with your document.
Step 2: With this handy PDF editing tool, it is possible to do more than merely complete blank fields. Express yourself and make your docs look faultless with customized textual content put in, or modify the original input to perfection - all supported by the capability to incorporate stunning photos and sign the document off.
This document will require specific information to be filled in, so you must take some time to fill in exactly what is required:
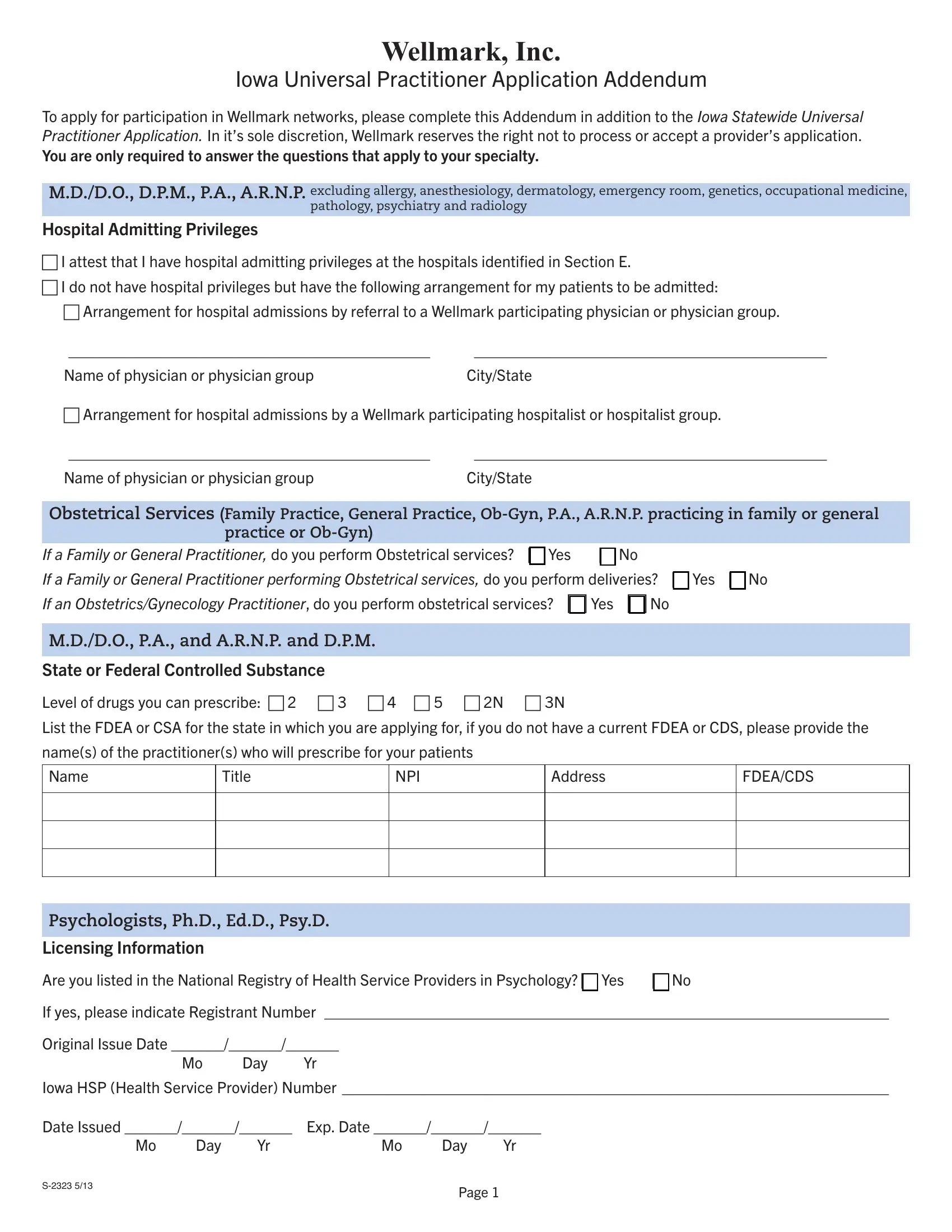
1. It is recommended to complete the hospitalist accurately, therefore take care while working with the parts containing these particular blanks:
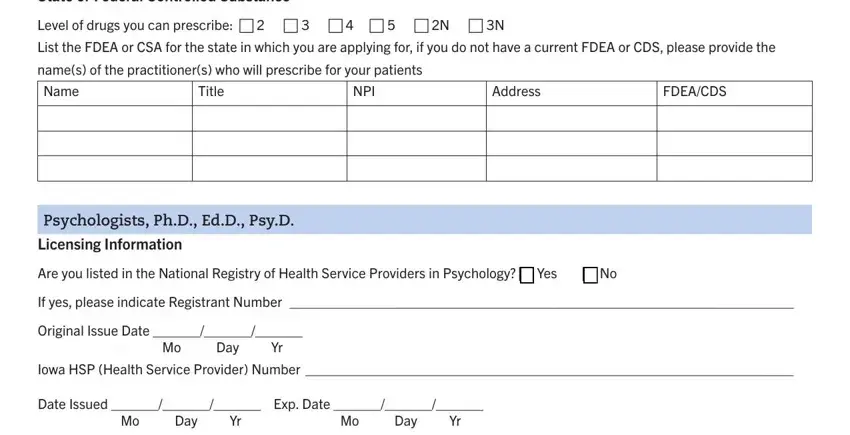
2. The next stage is usually to complete the next few blank fields: State or Federal Controlled, Level of drugs you can prescribe c, List the FDEA or CSA for the state, names of the practitioners who, Name, Title, NPI, Address, FDEACDS, Psychologists PhD EdD PsyD, Licensing Information, Are you listed in the National, If yes please indicate Registrant, Original Issue Date Mo Day Yr, and Iowa HSP Health Service Provider.
It's simple to get it wrong when completing your Are you listed in the National, for that reason be sure to go through it again prior to when you submit it.
3. In this step, have a look at Site Speciic Information If the, practice site, The following information is for, Group NPI, Credentialing Persons Title, Credentialing Fax Number TDD, Do you store electronic medical, Do you prescribe medication, Health Status, During the last three years have, If yes please explain, Are you unable with or without, Have you ever been required to, Malpractice, and Next Policy Period. These are required to be completed with highest awareness of detail.
4. To go onward, the next part requires typing in several form blanks. These comprise of Carrier Name, Policy Number Aggregate Amount, Efective Date End Date, Directory Information, List this site and specialty in, Reason not listed c No patient, c Other, BackUp Physician Information Blue, MDsDOs OBGYNs and PAsARNPs, Please list each individual, Name, Address, Specialty, NPI, and Efective, which you'll find vital to moving forward with this particular PDF.
5. The form should be wrapped up with this particular area. Further you'll see a full listing of blank fields that need accurate information in order for your document usage to be faultless: Page.
Step 3: Before moving forward, double-check that blanks were filled in correctly. Once you think it's all fine, click “Done." Download the hospitalist once you join for a free trial. Readily use the pdf within your FormsPal cabinet, with any edits and adjustments conveniently kept! We do not share any details you type in whenever completing forms at our site.