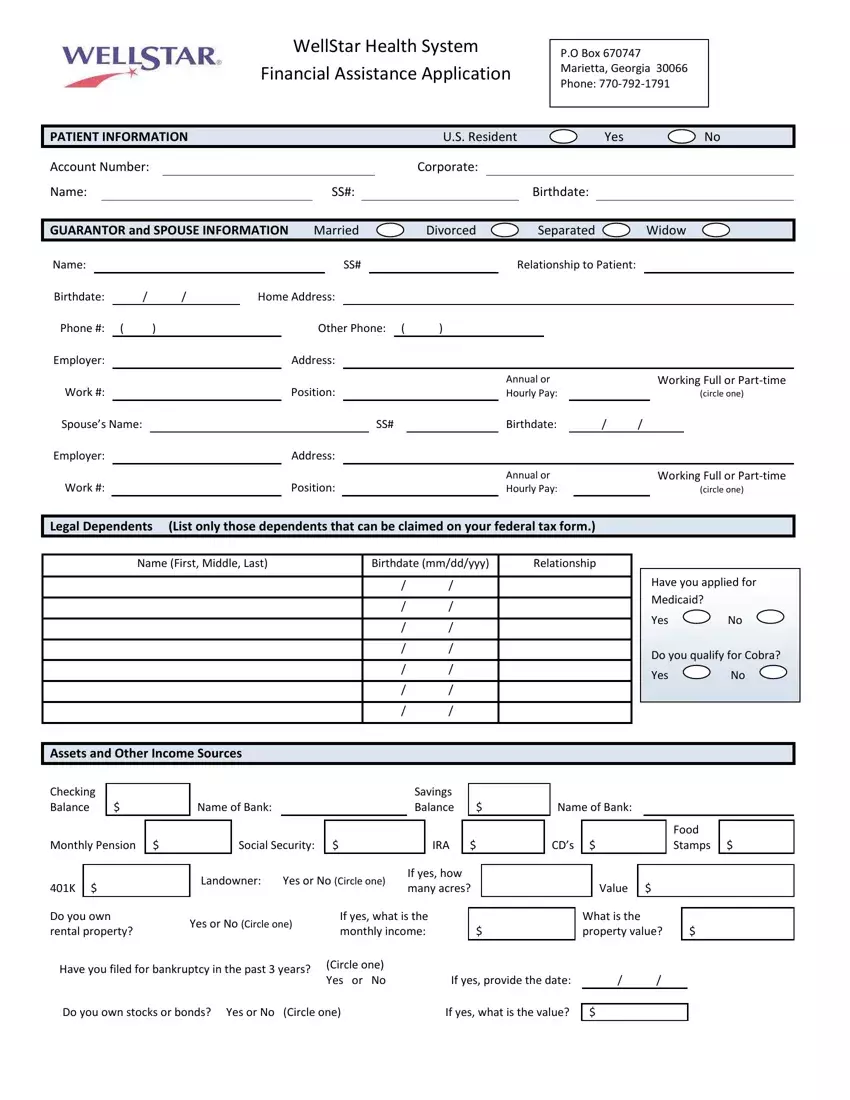
WellStar Health System
Financial Assistance Application
P.O Box 670747
Marietta, Georgia 30066
Phone: 770-792-1791
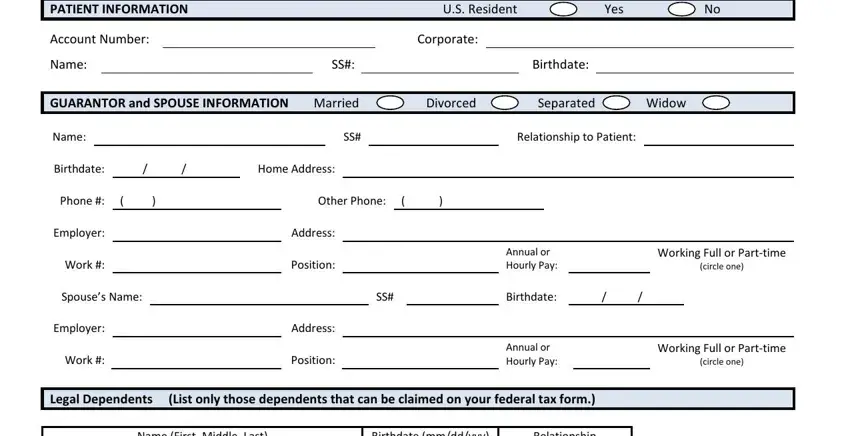
PATIENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
U.S. Resident |
|
|
|
|
Yes |
|
|
|
No |
Account Number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Corporate: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name: |
|
|
|
|
|
|
|
SS#: |
|
|
|
|
|
Birthdate: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
GUARANTOR and SPOUSE INFORMATION |
|
Married |
|
Divorced |
|
|
|
Separated |
|
|
Widow |
Name: |
|
|
|
|
|
|
|
|
|
SS# |
|
|
|
|
|
Relationship to Patient: |
|
|
|
|
Birthdate: |
|
/ |
|
/ |
Home Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone #: ( |
) |
|
|
|
|
Other Phone: ( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
Employer: |
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Annual or |
|
|
|
Working Full or Part-time |
Work #: |
|
|
|
|
|
|
Position: |
|
|
|
|
|
Hourly Pay: |
|
|
|
|
|
(circle one) |
Spouse’s Name: |
|
|
|
|
|
|
|
|
|
|
|
|
SS# |
|
|
|
|
|
Birthdate: |
|
/ |
/ |
|
|
|
Employer: |
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Annual or |
|
|
|
Working Full or Part-time |
Work #: |
|
|
|
|
|
|
Position: |
|
|
|
|
|
Hourly Pay: |
|
|
|
|
|
(circle one) |
|
|
|
|
|
|
|
Legal Dependents |
(List only those dependents that can be claimed on your federal tax form.) |
|
|
|
|
|
Name (First, Middle, Last) |
Birthdate (mm/dd/yyy) |
Relationship |
/ /
/ /
/ /
/ /
/ /
/ /
/ /
Have you applied for Medicaid?
Yes No
Do you qualify for Cobra?
Yes No

 Assets and Other Income Sources
Assets and Other Income Sources
|
|
|
|
Savings |
|
|
Name of Bank: |
|
Balance |
$ |
|
|
|
|
|
|
|
|
|
|
Social Security: |
$ |
|
IRA |
|
$ |
|
|
|
Landowner: |
Yes or No (Circle one) |
If yes, how |
|
401K |
$ |
many acres? |
|
|
|
|
|
Do you own |
Yes or No (Circle one) |
If yes, what is the |
|
|
|
|
|
|
rental property? |
monthly income: |
|
$ |
|
|
|
Have you filed for bankruptcy in the past 3 years? |
(Circle one) |
|
|
|
|
Yes or No |
|
If yes, provide the date: |
|
|
|
|
|
|
Value |
|
$ |
|
|
What is the |
|
|
|
|
|
|
property value? |
$ |
/ |
|
/ |
|
|
Do you own stocks or bonds? Yes or No (Circle one) |
If yes, what is the value? |
$ |
WellStar Health System is committed to providing financial assistance to patients who have sought medically necessary care at WellStar Health System but have limited or no means to pay for that care. WellStar Health will provide emergency medical care to all individuals, regardless of their ability to pay or eligibility under the Community Financial Assistance Policy.
In order to qualify for financial assistance, cooperation with WellStar Health is necessary in identifying and determining alternative sources of payment or coverage from public and private payment programs. In order to qualify for financial assistance, the following is necessary:
Required information:
Submit a true, accurate, signed and completed application for financial assistance; and
Provide a copy of the prior year Federal Income Tax Return and W2/1099 (including all schedules)
Provide two of the following if unable to provide a copy of the most recent Federal Income Tax Return:
Provide 3 months of the most recent pay stubs (or certification of unemployment); or
Separation Notice or unemployment claim if unemployed; or
Provide 3 current bank statements for all checking and savings accounts; or
Provide award letter from Social Security Office; or
Provide Current Profit and Loss report for all self-employed applicants; or
Current CD, 401k, 403b, IRA and other investment statements; or
Provide Asset Statement, with equity adjustments (Rental property, land, second houses)
This information must be received in order to process your application. If you fail to be compliant in returning the above information within 10 business days, WellStar Health System will not process your account for Community Financial Assistance approval. You may contact 678-838-5750 with questions.
Comments:
I hereby request that WellStar determine my eligibility for Community Financial Assistance. I understand that the information which I submit regarding my annual income and family size must be verified. I also understand that if the information I submit is determined to be false, such a determination will result in a denial of eligibility for Community Financial Assistance. I further agree to make application for any assistance (i.e., Medicaid, Medicare, State Aid (for cancer), Vocational Rehab, Insurance, etc.) that may be available for payment of my WellStar account charges. I will fully cooperate in taking whatever actions may be deemed necessary to obtain such assistance, and will assign or pay WellStar the amount recovered for WellStar charges. I agree to pay any balances remaining after the Community Financial Assistance adjustment is made. Failure to do so will result in a reversal of any Community Financial Assistance write-offs.
I affirm that the above information is true and correct to the best of my knowledge. |
|
|
|
Guarantor Signature: |
Date: |
|
|
Co-Guarantor Signature: |
Date: |
|
|
|
|
|