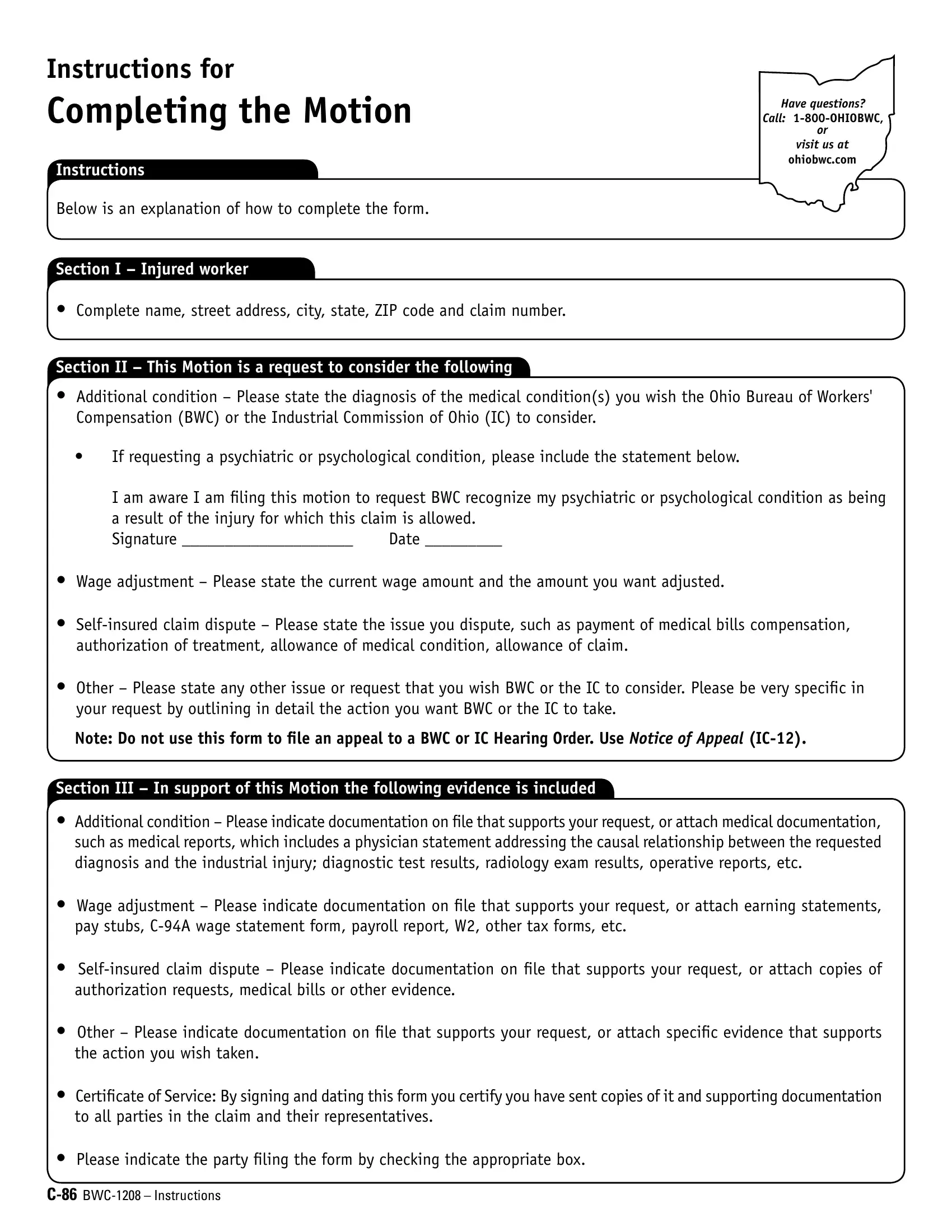
The C86 Motion for BWC form is an essential document for individuals involved in a claim with the Ohio Bureau of Workers' Compensation (BWC) or the Industrial Commission of Ohio (IC), particularly when specific actions by these organizations are requested that do not fall under standard forms or applications. This form caters to a variety of requests, such as disputes on self-insured claims, wage adjustments, or the recognition of psychiatric or psychological conditions as related to an injury claim allowed by BWC. To file this motion correctly, the party initiating the request must provide detailed information regarding the issue or adjustment being sought, including supporting documentation or evidence like medical reports, earning statements, or any relevant financial documents. It mandates the filer to certify service of the motion and supporting documents to all involved parties and outline clearly the evidence backing the request. Notably, healthcare providers or managed care organizations are directed to use different forms, emphasizing the C86 Motion's specific function for parties directly involved in a Workers' Compensation claim. This guide outlines how to complete the form and emphasizes the importance of submitting conclusive evidence to support the requested actions.
| Question | Answer |
|---|---|
| Form Name | BWC C-86 Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 28 |
| Avg. time to fill out | 6 min 10 sec |
| Other names | ohio bwc form c86, ohio c 86, ohio bwc c86, c 86 form |
Have questions? Call:
Motion
INSTRUCTIONS
•Parties to the claim requesting a decision by the Ohio Bureau of Workers' Compensation or the Industrial Commission of Ohio must use this form if any other form or application does not apply. Parties to the claim include the injured worker, employer and/or their authorized representatives and BWC. For a complete list of injured worker and employer forms visit ohiobwc.com, or call BWC at
•
•You must submit proof with this form to support the requested action. When requesting an additional condition, please include medical documentation, such as medical reports that include a physician statement addressing casual relationship between the requested condition and the industrial injury, diagnostic test results, radiology exam results, operative reports, etc. When requesting full or average weekly wage adjustments, include earning statements, such as pay stubs,
•The applicant must mail a copy of the Motion to all parties and/or their authorized representatives to the claim and will indicate a copy has been mailed by signing Certiicate of Service below.
CI |
Injured worker name |
Section |
Street address |
|
|
|
|
This Motion is a request to consider the following:
Claim number
City |
State |
|
|
|
|
Section II
In support of this Motion, the following evidence is included: (Please indicate the evidence included to support the request, such as medical reports that include a physician statement addressing casual relationship between the requested condition and the industrial injury, earning statements or any other evidence to support the requested action as outlined in the instructions.)
Section III
Certiicate of Service: I certify I have served a copy of this Motion on all parties and representatives to the claim.
Signed
Injured worker
Employer
Date signed
Authorized representative |
Administrator of the Ohio Bureau of Workers' Compensation |
Distribution: Original – Claim File |
Copies – as needed |