This Wisconsin Accident Form is used when no law enforcement officer is present to file a report and is required under significant property damage, injuries, or damage to government property. Below is a guide on how to correctly fill out this document.
1. Determine Eligibility
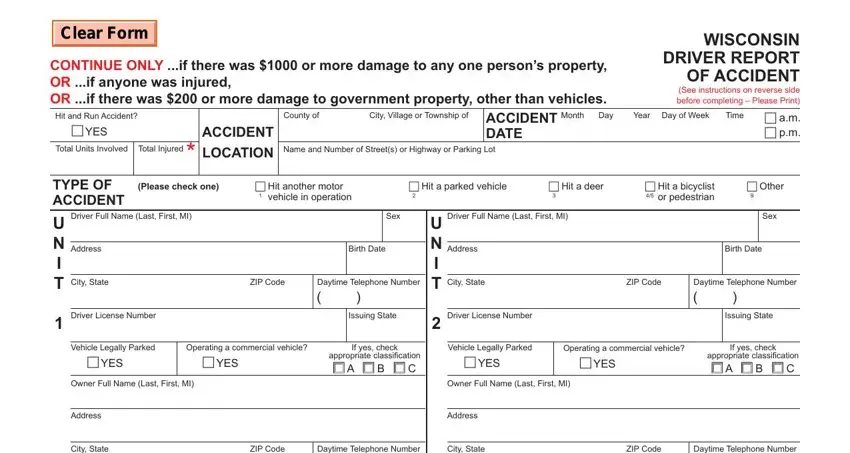
First, ensure no law enforcement officer has completed a report on the accident. You do not need to complete this form if an officer has filed a report. Otherwise, proceed if at least $1000 in damage to someone's property, any injury occurred, or $200 or more damage to government property.
2. Fill Out Your Information
As "Unit 1", provide all your details, including your full name, address, birth date, driver's license number, and contact information. If you own the vehicle, ensure that your vehicle's information, such as the license plate and vehicle identification numbers, are accurately recorded.
3. Provide Other Driver's Information
Include complete information for the other driver or property owner involved in the accident, referred to as "Unit 2". This includes their name, address, contact information, and details about their vehicle and insurance, if applicable.
4. Describe the Accident
Use the "Narrative" section to describe how the accident occurred. Be detailed in your explanation to ensure a clear understanding of the events. Additionally, a diagram of the designated area should be drawn to represent the accident scene. Include arrows to indicate directions and positions of the vehicles or properties involved.
5. Document Damage and Injuries
Detail any property damage and list injuries according to severity as categorized by codes A (Severe), B (Moderate), or C (Minor). If the space is insufficient, attach additional sheets of plain paper to accommodate all necessary information.
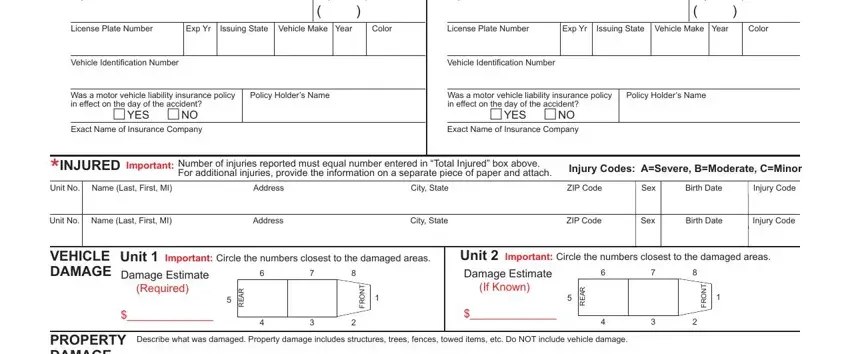
6. Verify Insurance Information
Confirm whether a car insurance policy was in effect during the accident. Provide the insurance company's name and the policyholder's name.
7. Review and Sign
Review the form to ensure all information is complete and accurate. Sign the form as required. It confirms that you have provided truthful and complete information to the best of your knowledge.
8. Mail the Form
Fold the report so that the address panel shows on the outside. Secure the bottom edge with tape (do not use staples) and mail it to the address provided on the form. Retain a copy of this report for your records.
