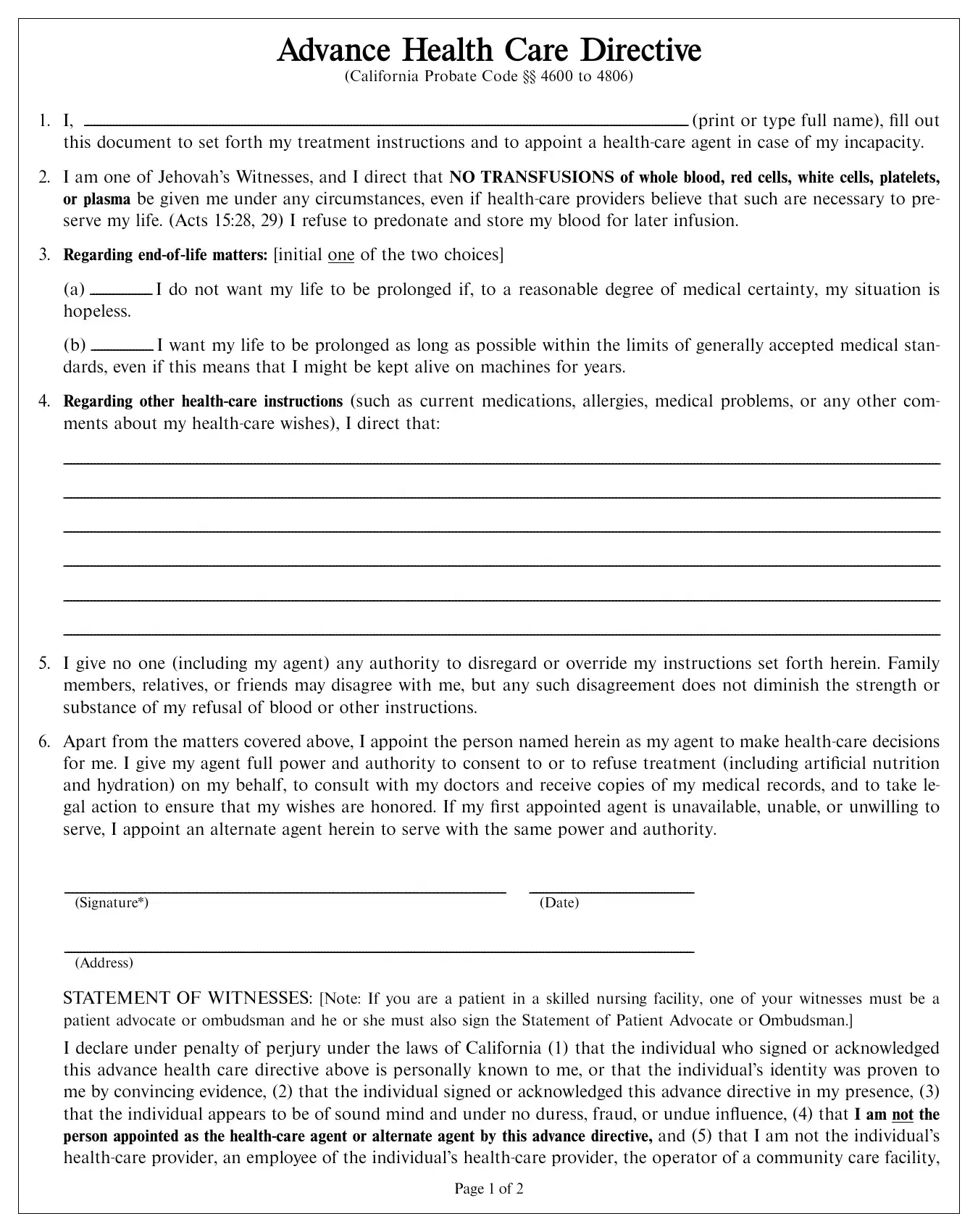
At the heart of every health care decision lies the fundamental right to direct one's own medical care, especially in circumstances that are deeply personal and, often, complex. The Advance Health Care Directive form, specifically as it pertains to members of Jehovah's Witnesses in California, embodies this principle by allowing individuals to outline their medical treatment preferences early on, particularly their refusal of blood transfusions under any circumstances. This document not only covers decisions about life-sustaining treatment but also appoints a health-care agent, granting them the authority to make decisions on the individual's behalf should they become incapable of doing this themselves. Beyond specifying medical treatment preferences, including the staunch refusal of blood transfusions, this Directive emphasizes the significance of choosing a health-care agent with care, detailing the person's full name, address, and contact information to ensure clarity and ease in critical moments. Furthermore, it sets strict witness requirements and outlines the legal implications for those appointed as agents or witnesses, ensuring the individual's wishes are both respected and protected. This comprehensive form serves as a critical tool for members of the Jehovah's Witness community to assert control over their health care in alignment with their religious beliefs and personal wishes, even in situations where they may not be able to communicate these themselves.
| Question | Answer |
|---|---|
| Form Name | Witness Dpa Card Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | jw no blood card pdf, no blood card jw, jw no blood card, printable no blood card |