
When using the online PDF editor by FormsPal, you'll be able to fill in or modify work form medical pdf here. Our team is continuously working to enhance the tool and help it become much better for users with its many features. Take advantage of the current modern opportunities, and find a heap of new experiences! Starting is easy! All that you should do is adhere to these basic steps down below:
Step 1: Click the "Get Form" button above. It's going to open our editor so that you can begin filling in your form.
Step 2: Once you access the file editor, you will see the form ready to be filled in. Other than filling in different blanks, you can also do other things with the form, including adding custom textual content, modifying the original text, adding images, putting your signature on the PDF, and a lot more.
This form will involve specific details; in order to ensure accuracy, make sure you heed the recommendations hereunder:
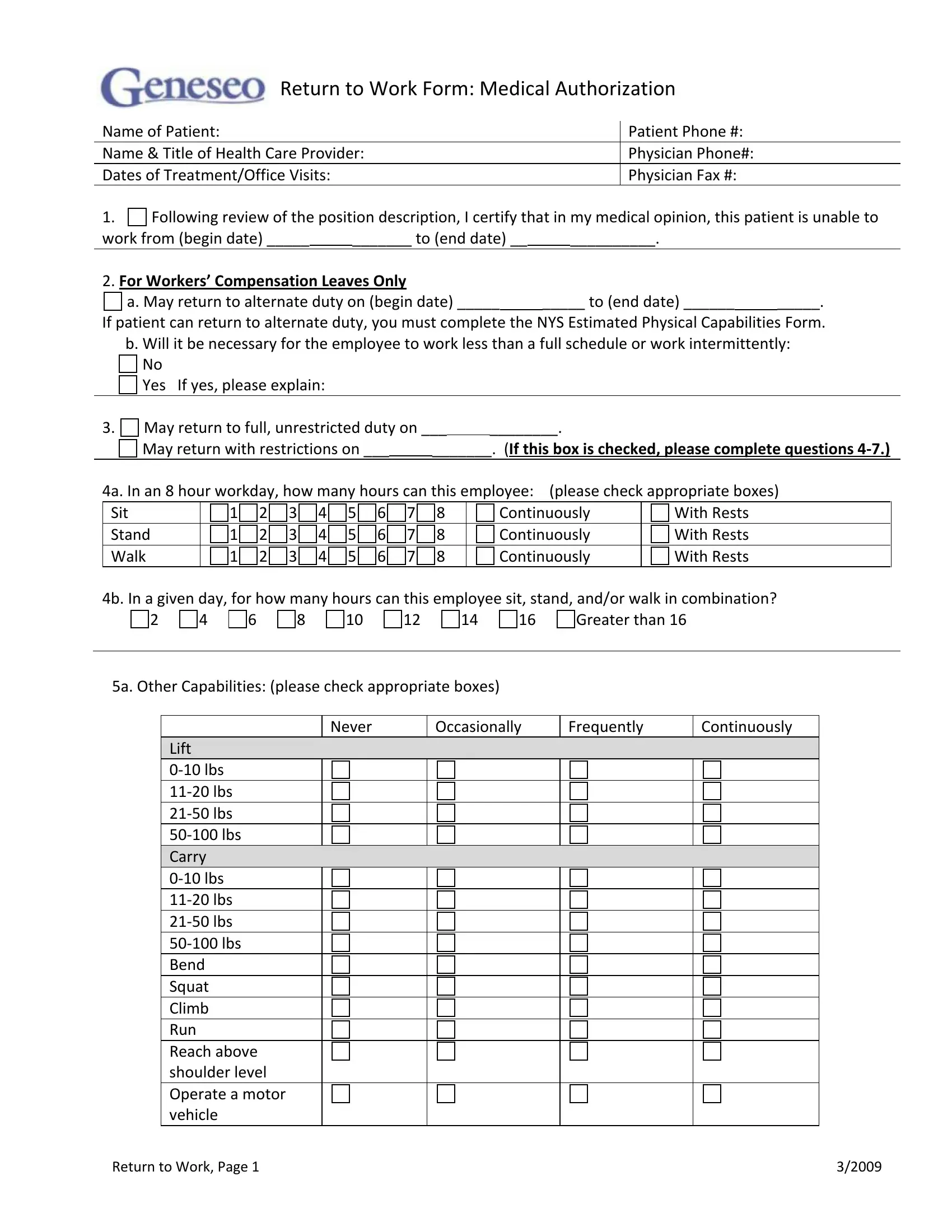
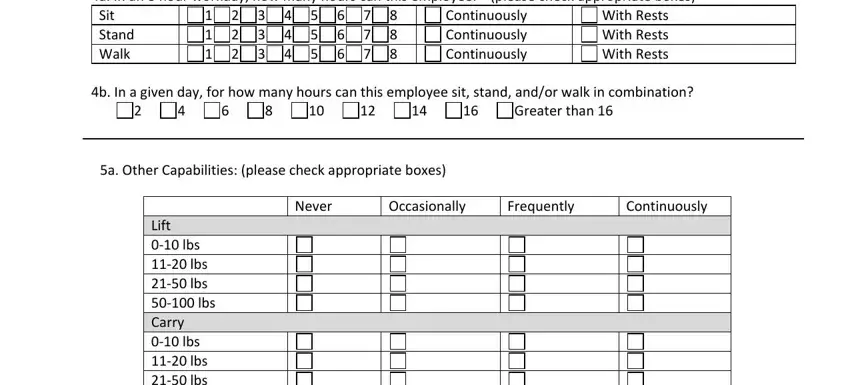
1. It's essential to complete the work form medical pdf correctly, thus be careful when filling in the sections including all of these blanks:
2. Your next step is usually to fill in the following fields: a May return to alternate duty on, Continuously Continuously, With Rests With Rests With Rests, b In a given day for how many, Greater than, a Other Capabilities please check, Lift lbs lbs lbs lbs Carry, Never, Occasionally, Frequently, and Continuously.
As to Lift lbs lbs lbs lbs Carry and Frequently, ensure you get them right in this section. Both these could be the key ones in the PDF.
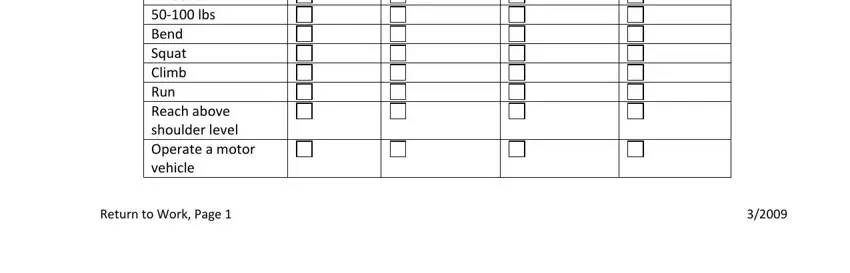
3. This next portion is focused on Lift lbs lbs lbs lbs Carry, and Return to Work Page - fill in every one of these empty form fields.
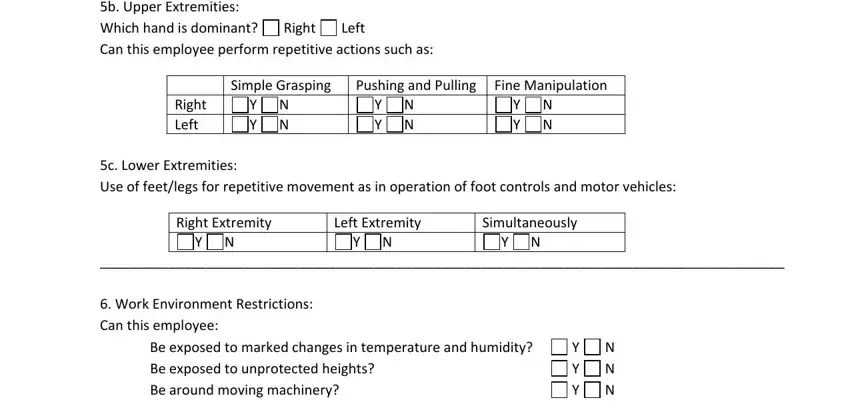
4. To go ahead, this section involves completing a handful of fields. Included in these are b Upper Extremities Which hand is, Right, Left, Right Left, Simple Grasping, Pushing and Pulling, Fine Manipulation, Y N Y N, Y N Y N, Y N Y N, c Lower Extremities Use of, Right Extremity, Y N, Left Extremity, and Y N, which you'll find essential to moving forward with this particular PDF.
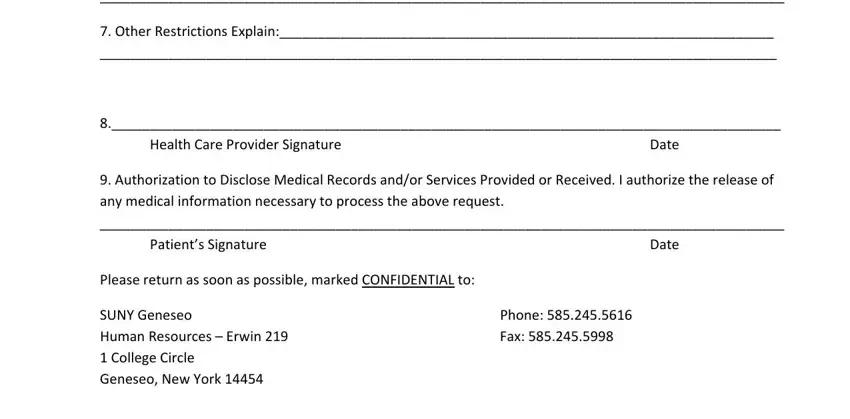
5. To conclude your form, this last area includes a few additional blank fields. Filling out Other Restrictions Explain, Health Care Provider Signature, Date, Authorization to Disclose Medical, Patients Signature, Date, Please return as soon as possible, Phone Fax, and SUNY Geneseo Human Resources will certainly finalize the process and you'll be done in a blink!
Step 3: As soon as you've reviewed the details entered, press "Done" to complete your FormsPal process. Grab your work form medical pdf after you register here for a free trial. Easily access the pdf document within your personal account, together with any modifications and adjustments all preserved! We don't share any information that you provide whenever filling out forms at FormsPal.