SSA Form SSA-3441-BK, known as “Disability Report – Appeal,” is required when an individual’s initial claim for disability benefits has been denied and they seek to appeal the decision. It collects updated information about the claimant’s medical condition, any new treatments, changes in daily activities, and work status since the last report was submitted. The form plays a critical role in providing the SSA with comprehensive and current details that might support the claimant’s case in the appeal.
The form is integral to the appeals process as it allows claimants to present new or additional evidence that could affect the outcome of their appeal. By filling out SSA Form SSA-3441-BK, individuals can document changes in their medical condition, including any worsening of their disability, new diagnoses, or changes in their ability to work and perform daily functions. This updated information is crucial for SSA reviewers to assess the continued eligibility or adjustment of benefits in light of the most recent health developments.
Other SSA Forms
Check a few other SSA PDF files accessible for editing in our editor. Additionally, keep in mind that it is easy to upload, fill out, and edit any PDF form at FormsPal.
Some filers may consider this template way too complex because they might be frightened about the number of pages. You will have to review and complete ten pages, providing a lot of data about yourself, your health state, and your representative (or a person who can be contacted to verify that you have a certain state).
The two first pages will be your instructions: reading them is compulsory to understand some peculiarities about the form and its completion. If you are unable to fill out the template on your own, ask your spouse, child, any other family member or relative, or friends who you trust to create the record for you. Another option is turning to SSA and asking their specialists for assistance.
In all cases, we provide the instructions below: they will guide you through the form step by step. Even if it seems confusing at the beginning, believe us, it will become easier the further you move.
The template is available on the SSA website. There, you can also submit the online document. However, since you are here, you can make use of our smart form-building software. It will prepare the fillable Form SSA-3441-BK for you in just a few seconds. When the template is ready, move forward to see what to do with it.
Read the Provided Info
This template starts with a bunch of instructions telling how to submit the document, what to add to some points you write, what you should do with your medical records, and so on. You must answer all questions included in the template.
You can either write all answers by hand or type them in using your laptop or PC. To each address, add a postal code; to each phone number, add its area code.
On the second page, you may find out how to file the document correctly. The contact phone number you can dial in case of questions is written here, too. Also, here you can learn about the use of personal data. SSA demands that you remove the first two pages from the form when you read everything (you have to submit only eight pages from 3 to 10).
Start Completing the Form
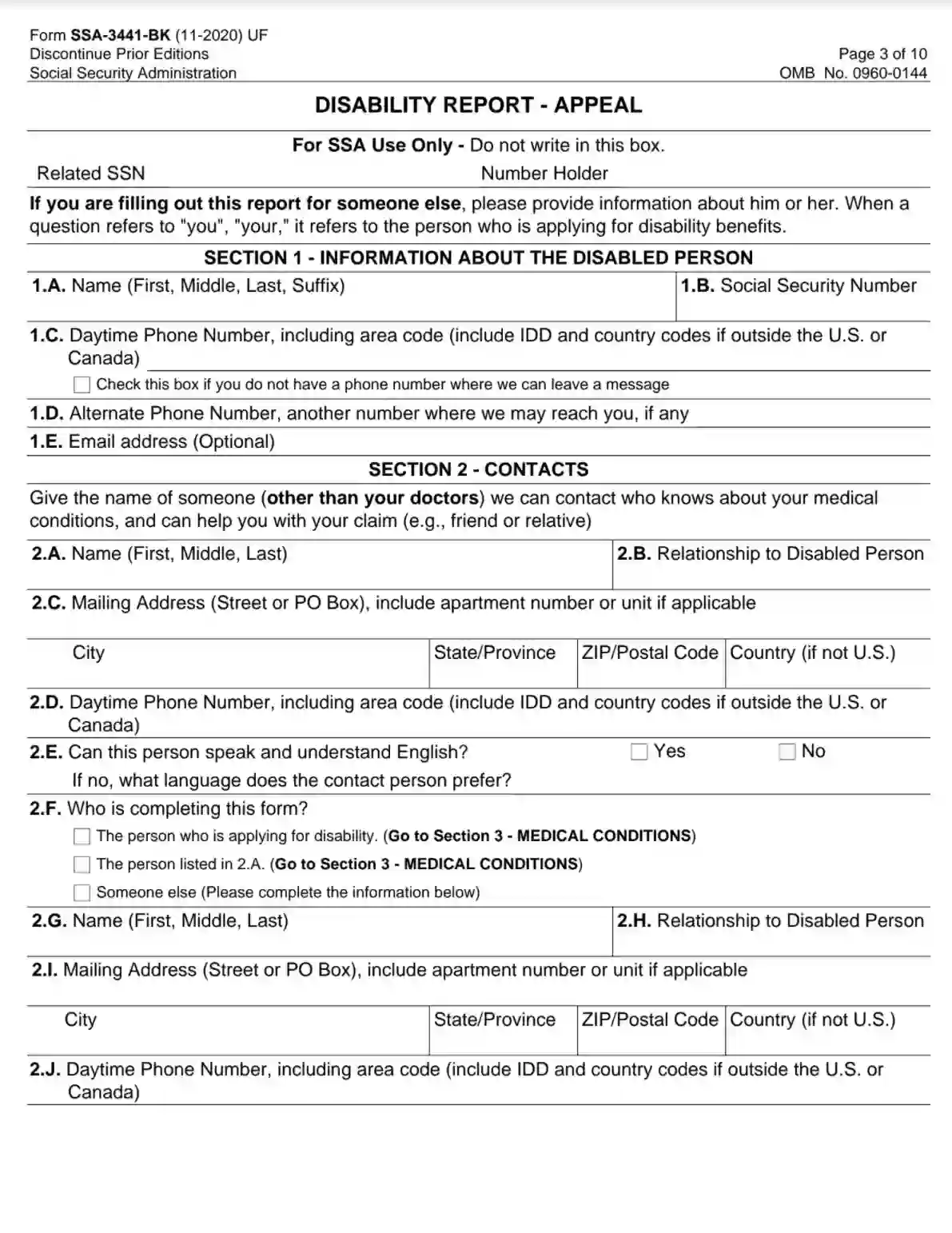
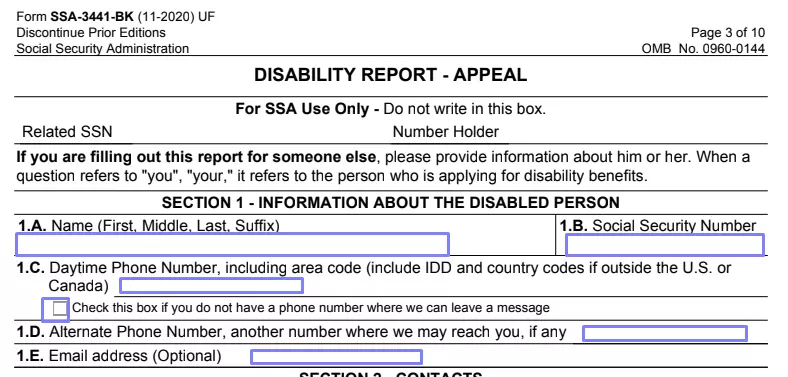
On Page 3 (or the first page where you will write something), you will see a block that SSA personnel will use for its purposes when it receives the document. You do not have to write anything there; so, move to Section 1 right away.
Write the disabled person’s full name, social security number (SSN), and daytime phone number. If there is no phone number they use, mark the box below the line where you are supposed to insert the number. Then, insert another phone number the claimant uses (if they have any) and their valid email address.
Provide the Applicant’s References
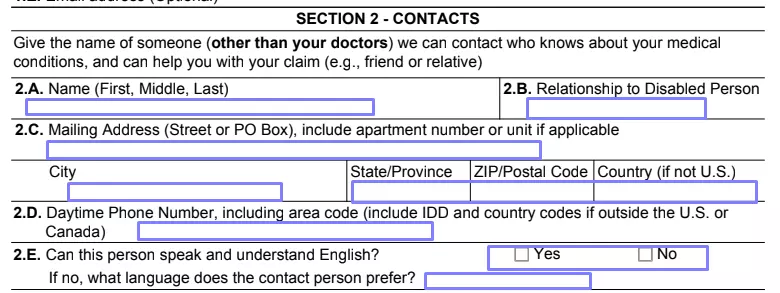
You have to add at least one person who is not the disabled person’s physician but someone who is aware of the disabled’s health condition and can verify that there are specific circumstances. It can be the disabled’s spouse, family member, close friend, colleague, or anyone else who knows about the situation.
Write this person’s full name, type of relationship to the claimant, mailing address (with a country, if not the United States), and phone number. Answer if the person speaks English. If not, indicate the preferred language.
Define who completes the template. If the disabled person or their representative mentioned above is doing it, mark the box and move to the following section. If it is a third party never mentioned in the form, this party has to write their details below: their full name, relationship to the claimant, mailing address, and telephone number.

Describe the Claimant’s Medical Conditions
The form’s Section 3 requires answering two questions about the disabled’s medical state. Answer if there are any changes in medical conditions or if the claimant has any new illnesses compared to the previously described facts. If the answer is “yes,” specify the dates when the changes occurred and provide details. You can also use the form’s last sheet to make comments.

Give Info on the Disabled’s Medical Treatment
The following section is quite long and is entirely about the claimant’s medical treatment. There is a set of questions accompanied by a couple of charts to fill out.
Answer if the claimant has ever used any other names than the one stated above. If yes, list all the names used. Then, in Line 4B, indicate if the claimant has had any appointments with their doctor (after their previous application had been declined) or they have planned appointments in the near future. Specify whether the disabled person will be seen by a doctor due to physical or mental issues.
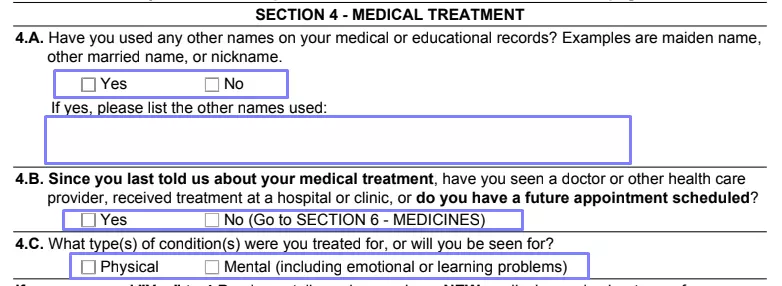
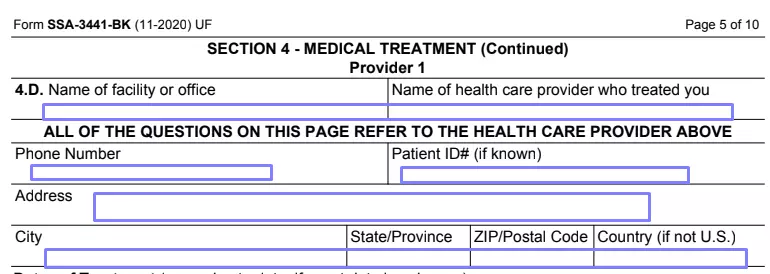
If you have answered affirmatively in Line 4B, you should add more info to the template because SSA will probably request the claimant’s medical records from those appointments. You can insert details about three care providers who currently treat the disabled person (hospitals, physicians’ offices, and others). Each of the three following pages describes one provider because many details are required.

For every provider, enter the facility’s or office’s name and the name of the person who has provided the claimant with treatment. Write this person’s phone number, Patient ID number (if you know it), and full address.
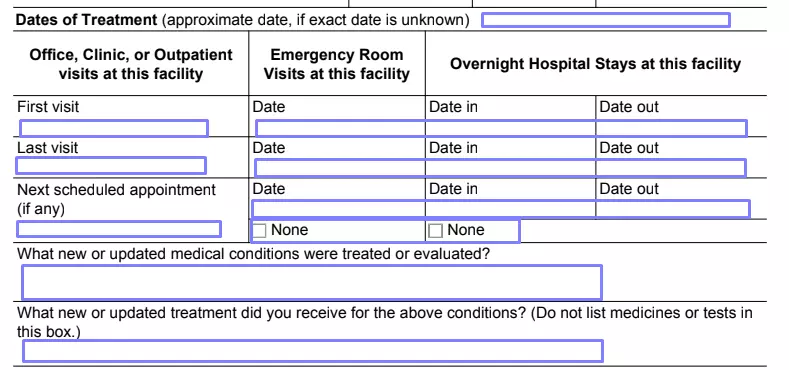
Fill out the chart that describes the dates of treatment. Insert all the needed dates (the claimant’s first and last visit, days of hospital stay, and emergency room attendance). List the new or updated medical conditions that were discovered or treated and the given treatment.
If the applicant has to do any tests and was told to do so by the provider, mark the “yes” box and all the applicable tests (EKG, EFG, breathing test, blood test, hearing test, and so on) in the table below. If you need more space to describe tests, use the form’s last page again.

Give the same details about all providers the claimant has consulted recently or will consult in the near future.
Specify Other Medical Info
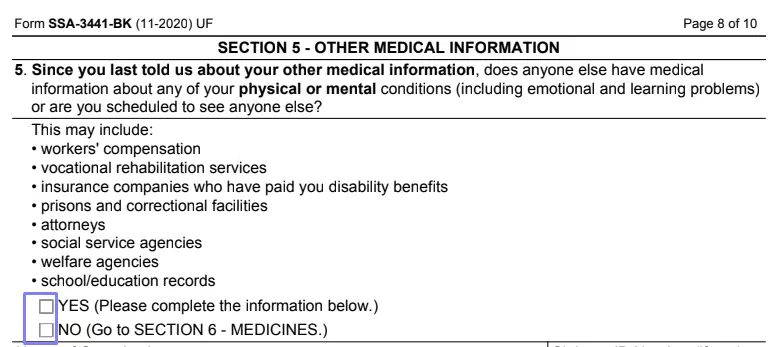
In Section 5, you are obliged to provide other medical details. You will see a list of other parties who may have access to the applicant’s medical info and plan to see the applicant soon. Among these parties are attorneys, social service agencies, prisons, insurance companies, and other organizations.
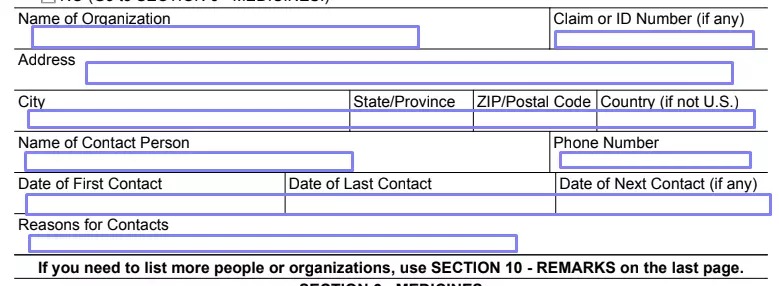
If the answer is no, mark the relevant box and move to the next section. If the answer is “yes,” mark the “yes” box and specify the organization or person by writing the organization’s name and address, the Claim or ID number (if any), contact person’s name, phone number, the dates of first, next, and last contact, and reasons for such contacts. Use the last sheet if you need more space.
Tell about the Claimant’s Medication
First, answer if the applicant is taking any medicine right now. If no, go to the next section. If yes, for each medicine, add its name, the name of the physician who has prescribed it, the reason to take it, and side effects (if any). If the chart is not enough to describe all pills the claimant is taking, move to the form’s last sheet and continue writing there.

Reply about the Applicant’s Activities
You should describe any changes that have happened to the claimant’s daily activities since they have turned to SSA for the last time. If there are no changes, mark the “no” box and proceed to the following section.
Describe the Applicant’s Work and Education Situation
Answer the questions about the applicant’s work (if it has changed or not). Tell about the attended classes with the dates of attendance and the received degree.

Answer about Support Services
If the applicant has taken part in any support services described in the form, provide the required details. The services’ list is added here so you can easily understand whether it is the applicant’s case or not. Provide the organization’s name, the coach or counselor’s name, their phone number, and the organization’s address. Insert the date when the applicant started to participate in the program.

Provide Comments and Remarks
We have mentioned the last sheet before — you can use it to add more info for each section. If you have something more to add and you consider that the SSA must know about it, write the information here. On the bottom of this sheet, write the current date (the date when you are completing this template).