Advance Beneficiary Notice of Non-coverage (ABN) is a notice given to Medicare beneficiaries to convey that Medicare is not likely to provide coverage for a specific medical service, procedure, or item. Healthcare providers or suppliers provide this document before delivering a service or item expected to be denied by Medicare based on issues of necessity or coverage restrictions. It informs the patient about their potential financial responsibility. It allows them to decide whether to proceed with the service, knowing they might have to bear the cost.
When a provider issues an ABN, it must clearly explain why Medicare might deny the payment. The patient then has the option to accept or refuse the recommended services or items. If they choose to proceed, they sign the ABN, acknowledging their understanding and agreement to pay out-of-pocket should Medicare deny coverage.
Other Financial Forms
Should you wish to check out more financial PDFs that you can edit and fill in online, below are some of the more popular forms among our visitors. Moreover, remember that you can easily upload, fill out, and edit any PDF form at FormsPal.
When you receive this form, you can choose a suitable alternative from the suggested ones. Let’s investigate all of them one by one:
Once you decide which particular option you want to choose, completion of the form will be easy for you. Here is a detailed guide on filling out this form line-by-line.
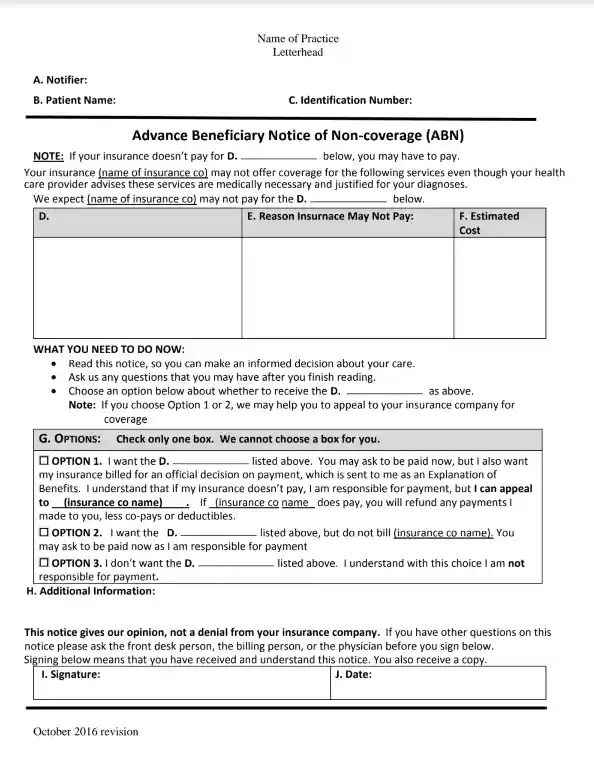
Enter personal info about the notifier
The first line of the form requires the name, physical address, and phone number of the notifier — provider of the form. It can be your physician or another person who is eligible to give this document to you. Besides, this part of the form should be filled by notifier and fields B and C.
Introduce patient
Lines B and C are prepared for the data about the patient or beneficiary. In the first field, a doctor should write the patient’s name, and in the second one, his or her identification number. You can skip the field with the identification number because it is not obligatory to fill it.
Clarify paid service or item
You should enter the category of provided service inbox D. Make sure you use one of these names:
You should not put the service or product’s full name here because you will describe it later in the table.

Fill in the table
Clarify the name of the paid procedure or item in column D, then enter the reason why Medicare will not pay for it based on what is described above in column E. Do not forget to enter the approximate amount you will need to pay for this service in column F.
Enter type of service
In field D under the table, you should once again fill the category of the product or service that Medicare denied paying for.

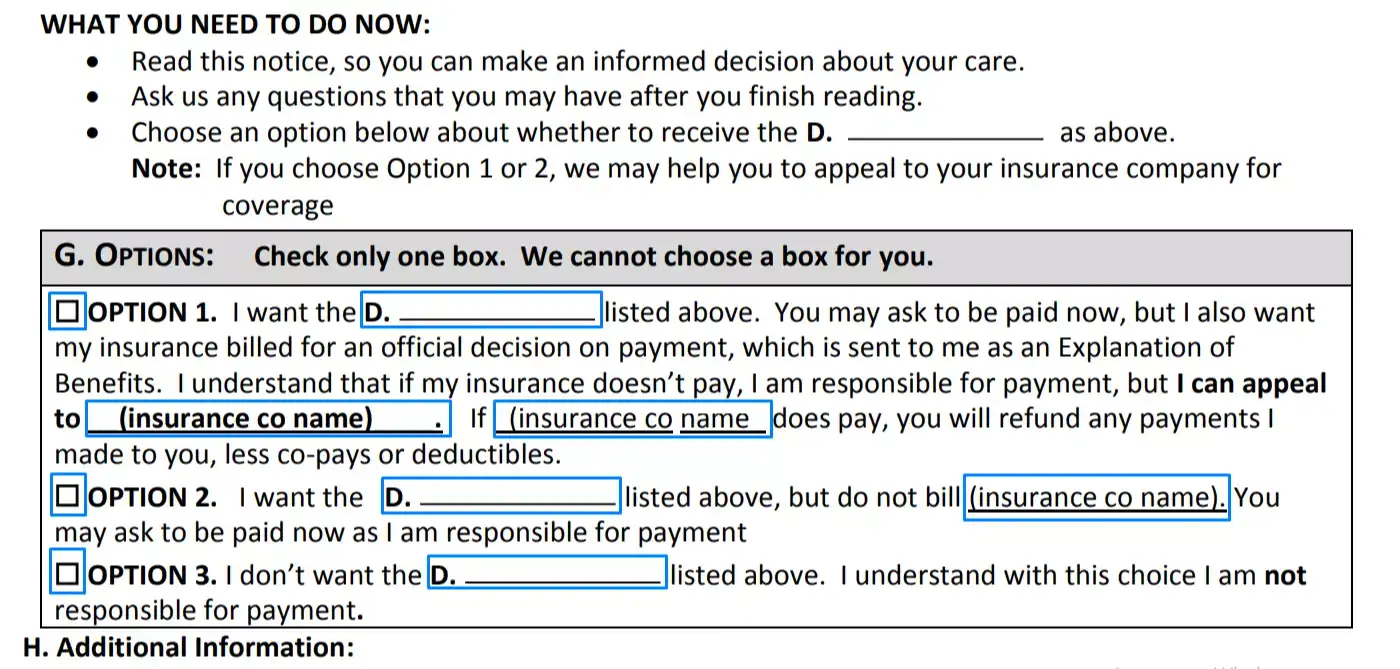
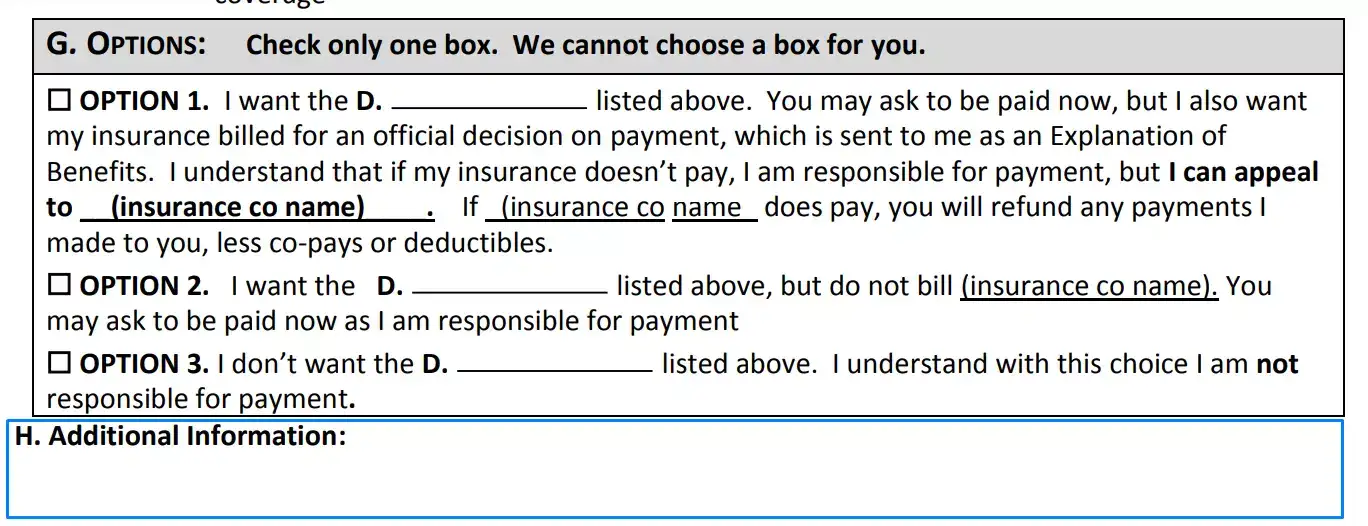
Choose suitable option
Then you should put a checkmark in the box near the alternative that you want to select. Make sure you write in the category of the provided services here near letter D. Fill the blanks in the text for chosen option only. If it is required here to write the name of the insurance company, do not forget to do this.
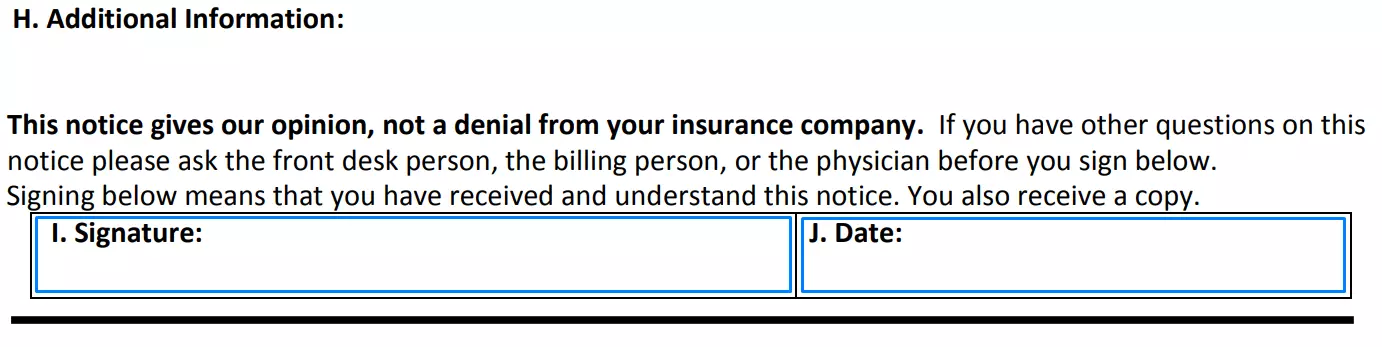
Provide additional information (optional)
If you, as a beneficiary, do not want to select one of the options, you should provide additional data in field H.
Sign the form
At the end of the form, you should put your signature and date of completion as an agreement with offered conditions.
After the filling out, you should give the advance beneficiary notice to the notifier. If you choose the first alternative, it will take some time to get the answer from Medicare. You will need to make a fee for the medical procedure, but they will return your money if they agree with your claim.