
When working in the online PDF editor by FormsPal, you can complete or edit the AAA Form AR right here in your browser. Here is how to get started:
Step 1: Click the "Get Form" button above to open the PDF editor and begin filling in your arbitration request form.
Step 2: The tool lets you customize the form in many ways. Add your information, modify existing entries, and include a digital signature.
To finalize your AAA Form AR, complete the required fields in every section:
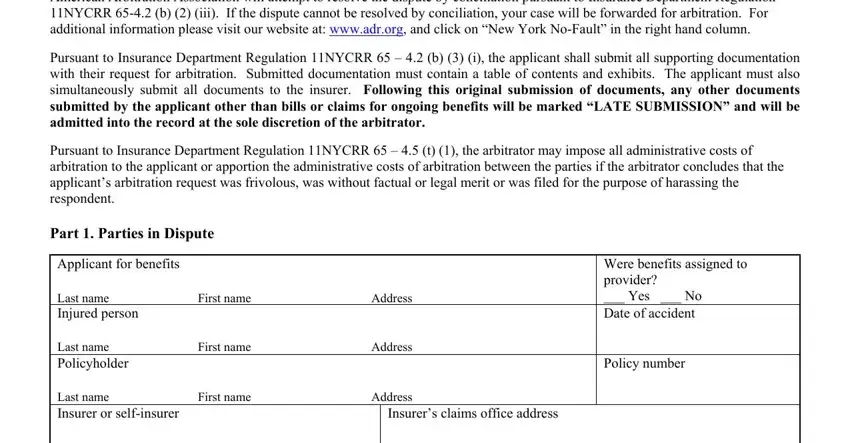
1. Enter the applicant and claimant details in the first section, including name, address, and contact information:
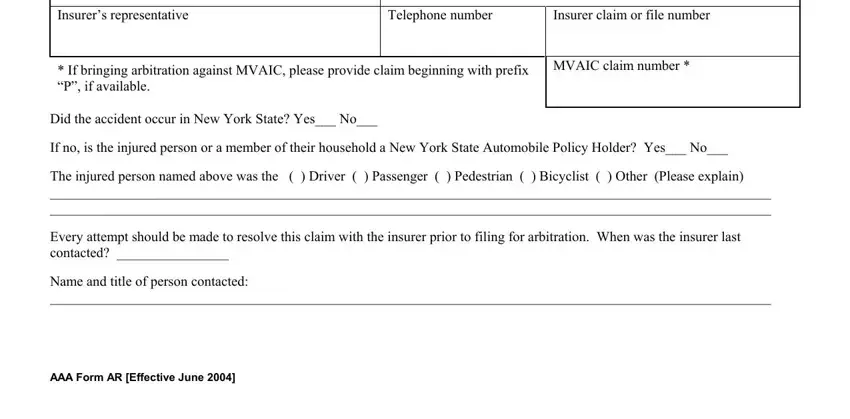
2. Complete the insurance details: Insurer representative, Telephone number, Insurer claim or file number, MVAIC claim number, and whether the accident occurred in New York State.
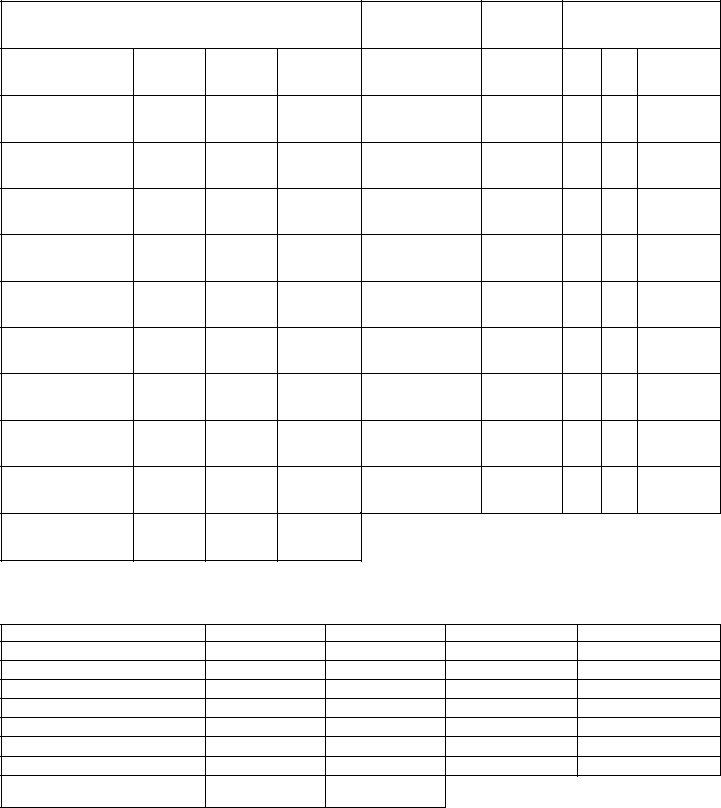
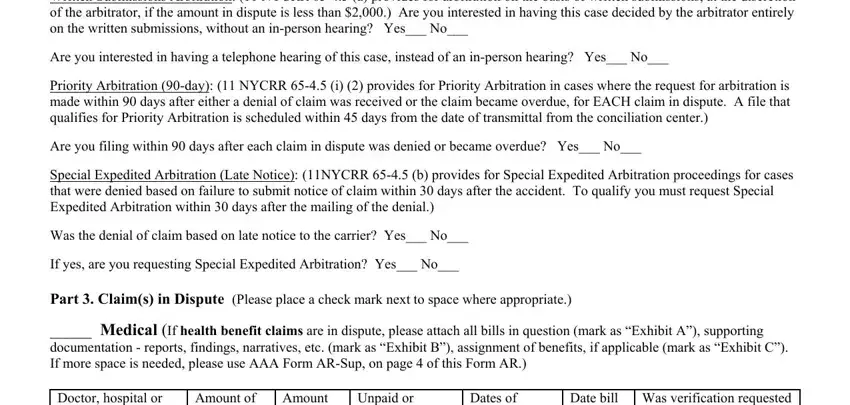
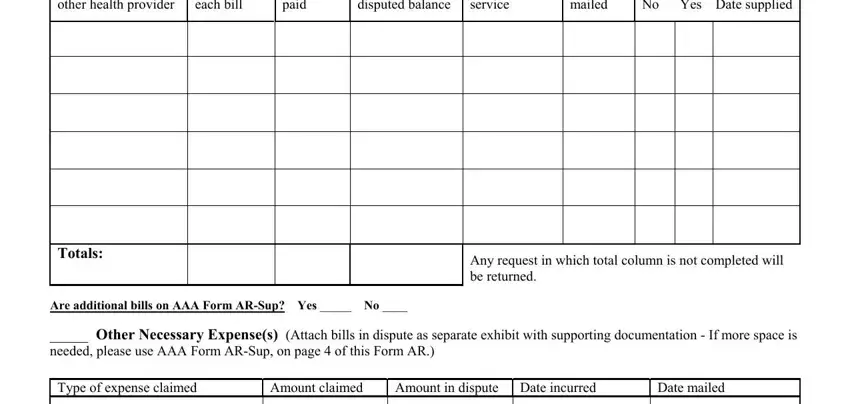
3. In Part 1 - Special Bills, enter: Doctor or hospital name, Amount of each bill, Amount paid, Unpaid or disputed balance, Dates of service, Date bill mailed, and whether verification was requested.
4. In the additional expense sections, fill in all expense types claimed, amounts, dates incurred, and verification details. Double-check unpaid balances and provider information - these fields are the most common source of errors.
5. Complete the final section with all remaining expense types, totals, dates, and additional AAA form items. Missing any required field may result in an incomplete submission.
Step 3: Review all fields before finishing. Click "Done" to finalize your AAA Form AR. Create a free account to save and manage your completed forms in your FormsPal cabinet.