In an increasingly complex healthcare landscape, the ABN (Advanced Beneficiary Notice) Commercial Insurance form serves as a critical document bridging the gap between healthcare providers, patients, and insurance carriers. This form is instrumental in facilitating the payment process for medical services under Medicare, elucidating the financial responsibilities and insurance requirements of the involved parties. It requires the patient's consent for the release of medical information necessary for claims processing, thereby adhering to privacy regulations. By stipulating that the patient agrees to be financially accountable for deductible, coinsurance, and non-covered services, which are determined by the insurance carrier's charge determination, the form sets clear expectations regarding payment. Additionally, it captures essential information such as insured name, relationship to patient, employer details, and insurance carrier information, ensuring that all requisite data for processing the medical and vision insurance claims are accurately recorded. Furthermore, the ABN form underscores the importance of the patient's understanding of their insurance plan, including the requirement to notify staff of insurance specifics to prevent unforeseen charges. The provision to file insurance claims or take assignment of benefits on behalf of the patient without additional fees highlights the patient-centric approach of healthcare providers. However, it firmly places the onus on patients to be aware of their insurance benefits and to provide proper identification to facilitate this process. Failure to comply with these requirements might render the patient liable for all charges, emphasizing the critical nature of this document in the healthcare billing and insurance domain.
| Question | Answer |
|---|---|
| Form Name | Abn Form Commercial Insurance |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | commercial abn, commercial insurance abn, commercial abn forms, abn form for commercial insurance |
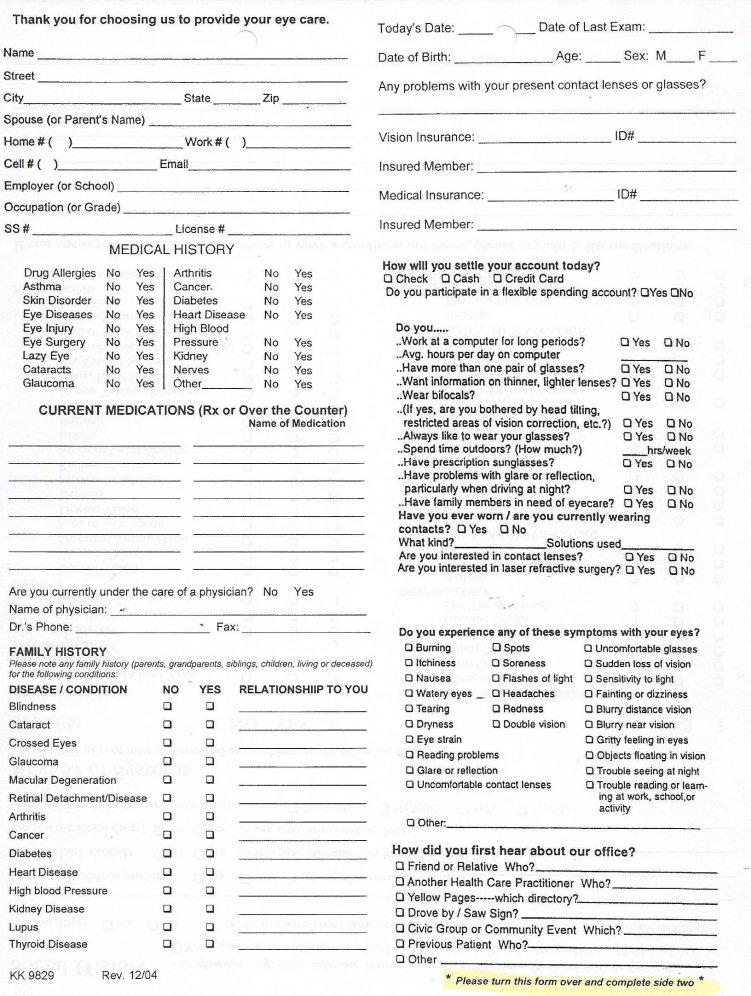
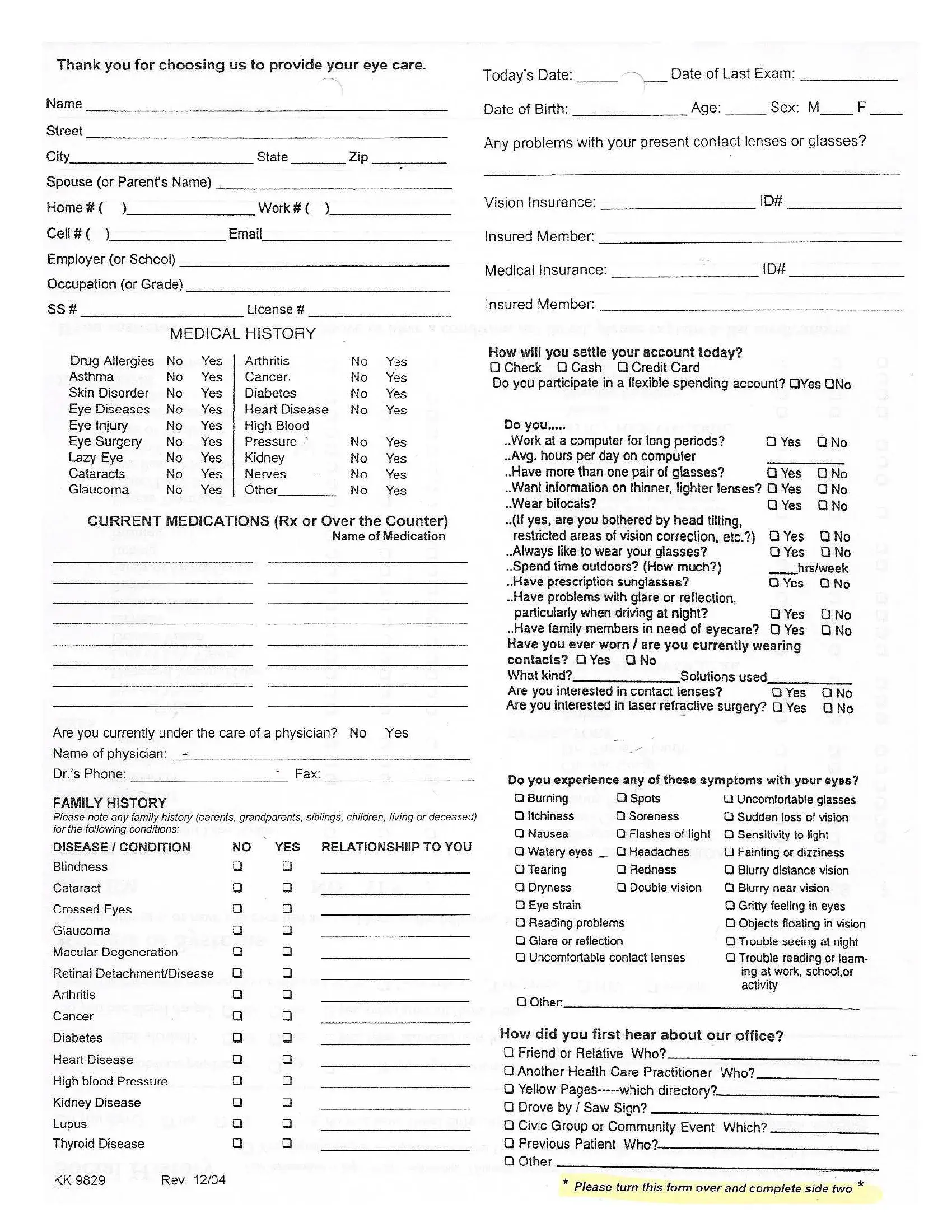
SIGNATURE ON FILE/ABN FORM
I request that payment of authorized Medical/Medicare Insurance benefits be made on behalf of (patient’s name)
_______________________________, for services furnished to me by Dr. Latham/Dr.
holder of medical information about me, to be released to the Centers for Medicare and Medicaid Services and its agents. Including any information needed to determine these benefits or the benefits payable to related services. I understand my signature requests that payment be made and authorizes release of medical information necessary to pay the claim. If other health information is indicated in Item 9 of the CMS 1500 form or elsewhere on other approved claim forms, my signature authorizes releasing the information to the insurer or agency shown. Dr Latham/Dr.
VISION INSURANCE
Insured Name(Mr./Mrs./Ms.) ________________________________ Relationship To Patient _________________________________
Insured’s Employer _______________________________________ Insured Date of Birth ___________________________________
Insured SS# _____________________________________________ Name of Ins. Carrier ____________________________________
Member ID# ____________________________________________ Group # ______________________________________________
MEDICAL INSURANCE
Insured Name(Mr./Mrs./Ms.) ________________________________ Relationship To Patient _________________________________
Insured’s Employer________________________________________ Insured Date of Birth ___________________________________
Insured SS# _____________________________________________ Name of Ins. Carrier ____________________________________
Member ID# ____________________________________________ Group # ______________________________________________
INSURANCE REQUIREMENTS
We will be happy to file your insurance claim forms or to take assignment of your vision and/or medical benefits as designated by your insurance company. We are happy to provide this service without any additional charge to you. We will do all that we can to help you receive the maximum benefits. However it is your responsibility to know your insurance plan’s requirements and benefits and to notify the staff at Harwood Vision Clinic. Lack of proper identification could result in you being responsible for all charges, and insurance claims will not be submitted after services have been rendered. We will gladly supply you the proper paperwork for you to submit your claim.
We go to great lengths to verify the amount and type of coverage you are allowed under your plan. We can quote your estimated coverage, however final determination of benefits will not occur until the insurance company receives your claim. In the event the plan sponsor determines that you are not eligible at the time of service, or determines that you are eligible for a reduced benefit level, or applies the charges to the deductible, by signing this statement you agree to be financially responsible for any and all charges incurred by you and not paid by the plan sponsor. Any balance on your account is due within 30 days. If not, a monthly finance charge of 18% will apply.
PRIVACY PRACTICES AND FINANCIAL RESPONSIBILITY
I acknowledge that a copy of Harwood Vision Clinic’s Privacy Practices has been made available to me. I agree to be financially responsible for any fees incurred as a result of today’s services and/or materials provided, including those not covered by insurance.
Signature ___________________________________________________ Date _________________________________________