Our PDF editor was designed with the purpose of making it as simple and user-friendly as possible. These particular steps will help make filling in the acord 130 fillable fast and simple.
Step 1: Choose the orange "Get Form Now" button on the following web page.
Step 2: As soon as you've entered the editing page acord 130 fillable, you should be able to discover all of the actions available for the document at the top menu.
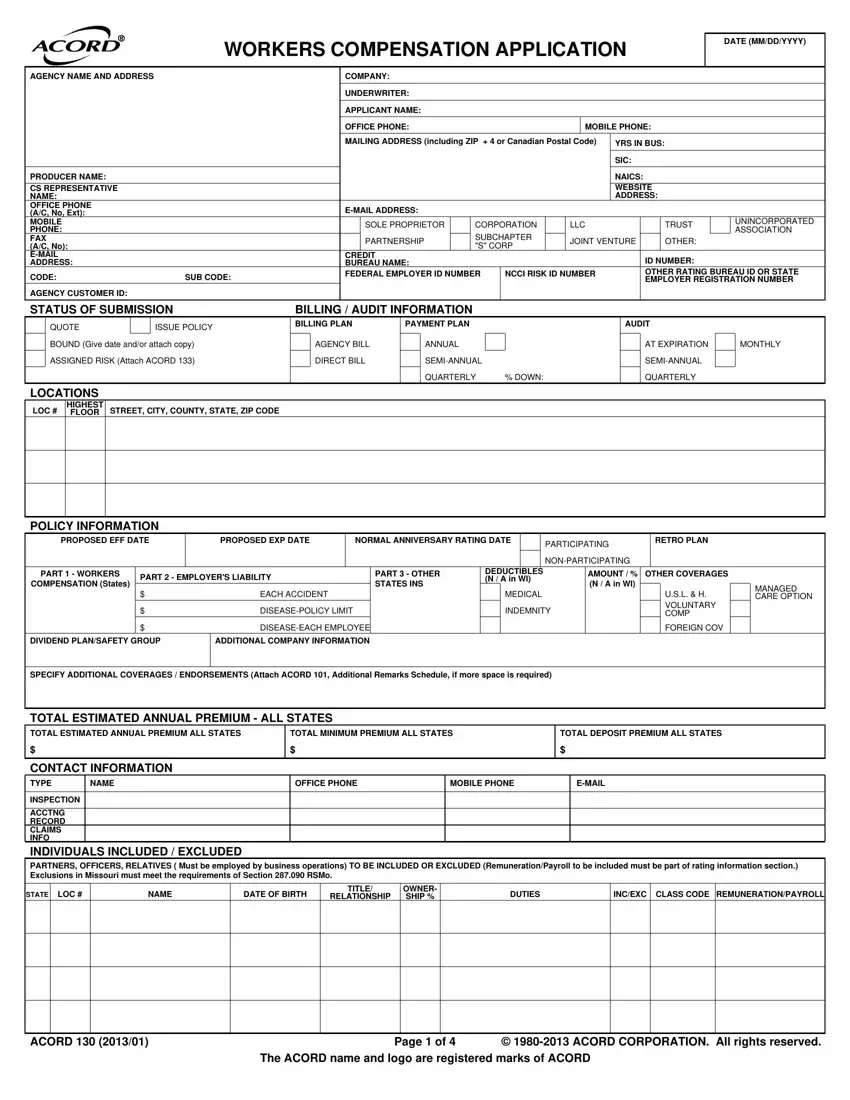
Fill out the acord 130 fillable PDF and type in the information for each and every area:
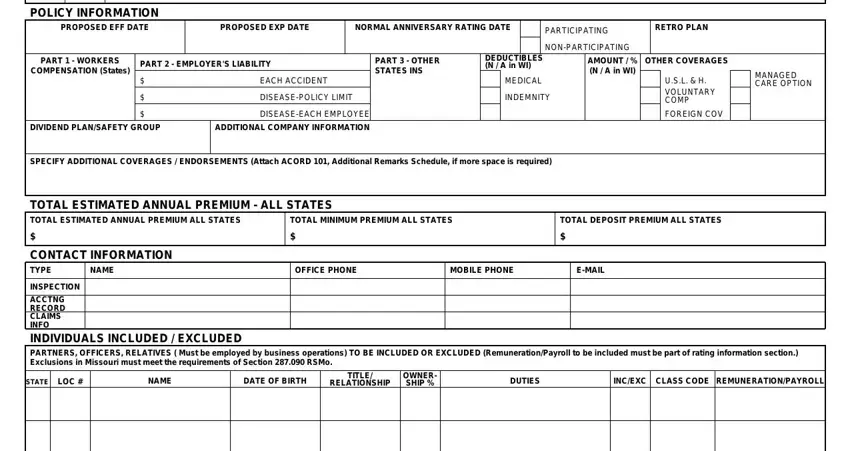
In the POLICY INFORMATION, PROPOSED EFF DATE, PROPOSED EXP DATE, NORMAL ANNIVERSARY RATING DATE, PARTICIPATING, NONPARTICIPATING, RETRO PLAN, PART WORKERS COMPENSATION States, PART EMPLOYERS LIABILITY, PART OTHER STATES INS, EACH ACCIDENT, DISEASEPOLICY LIMIT, DISEASEEACH EMPLOYEE, DIVIDEND PLANSAFETY GROUP, and ADDITIONAL COMPANY INFORMATION box, note down your data.
The application will request information to quickly submit the segment ACORD, Page of The ACORD name and logo, and ACORD CORPORATION All rights.

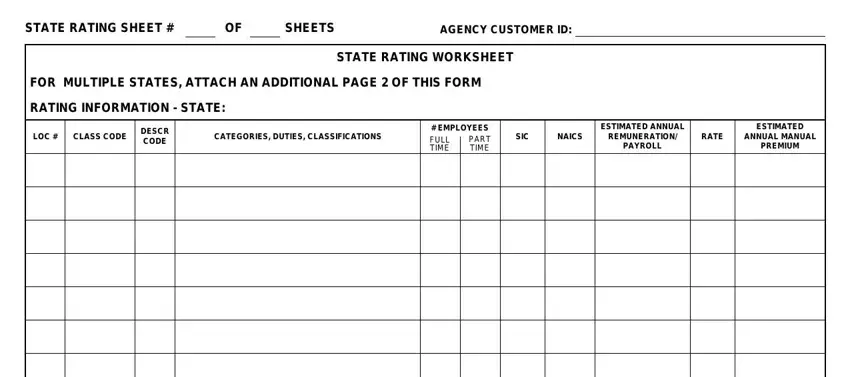
Make sure you describe the rights and obligations of the sides inside the STATE RATING SHEET, SHEETS, AGENCY CUSTOMER ID, FOR MULTIPLE STATES ATTACH AN, RATING INFORMATION STATE, STATE RATING WORKSHEET, LOC, CLASS CODE, DESCR CODE, CATEGORIES DUTIES CLASSIFICATIONS, EMPLOYEES PART FULL TIME TIME, SIC, NAICS, ESTIMATED ANNUAL REMUNERATION, and RATE part.
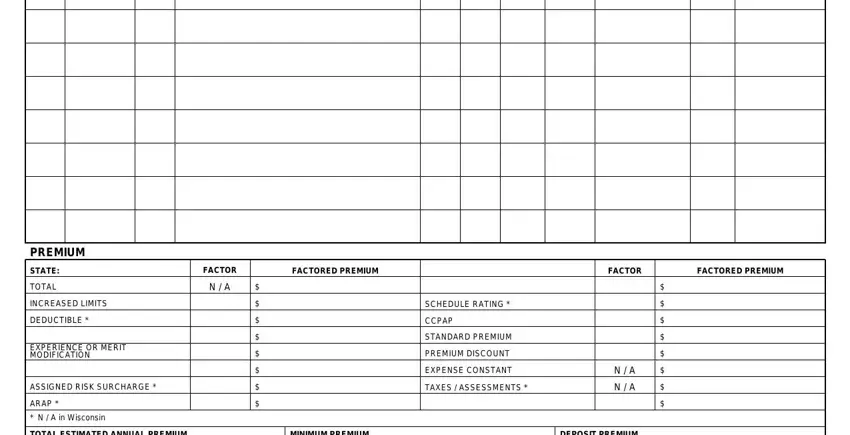
Finish by checking the following sections and preparing them as required: PREMIUM, STATE, TOTAL, INCREASED LIMITS, DEDUCTIBLE, EXPERIENCE OR MERIT MODIFICATION, ASSIGNED RISK SURCHARGE, ARAP, N A in Wisconsin, FACTOR, N A, FACTORED PREMIUM, FACTOR, FACTORED PREMIUM, and SCHEDULE RATING.
Step 3: As soon as you've hit the Done button, your document will be readily available transfer to any kind of device or email you indicate.
Step 4: Be sure to generate as many copies of the form as you can to avoid potential troubles.
