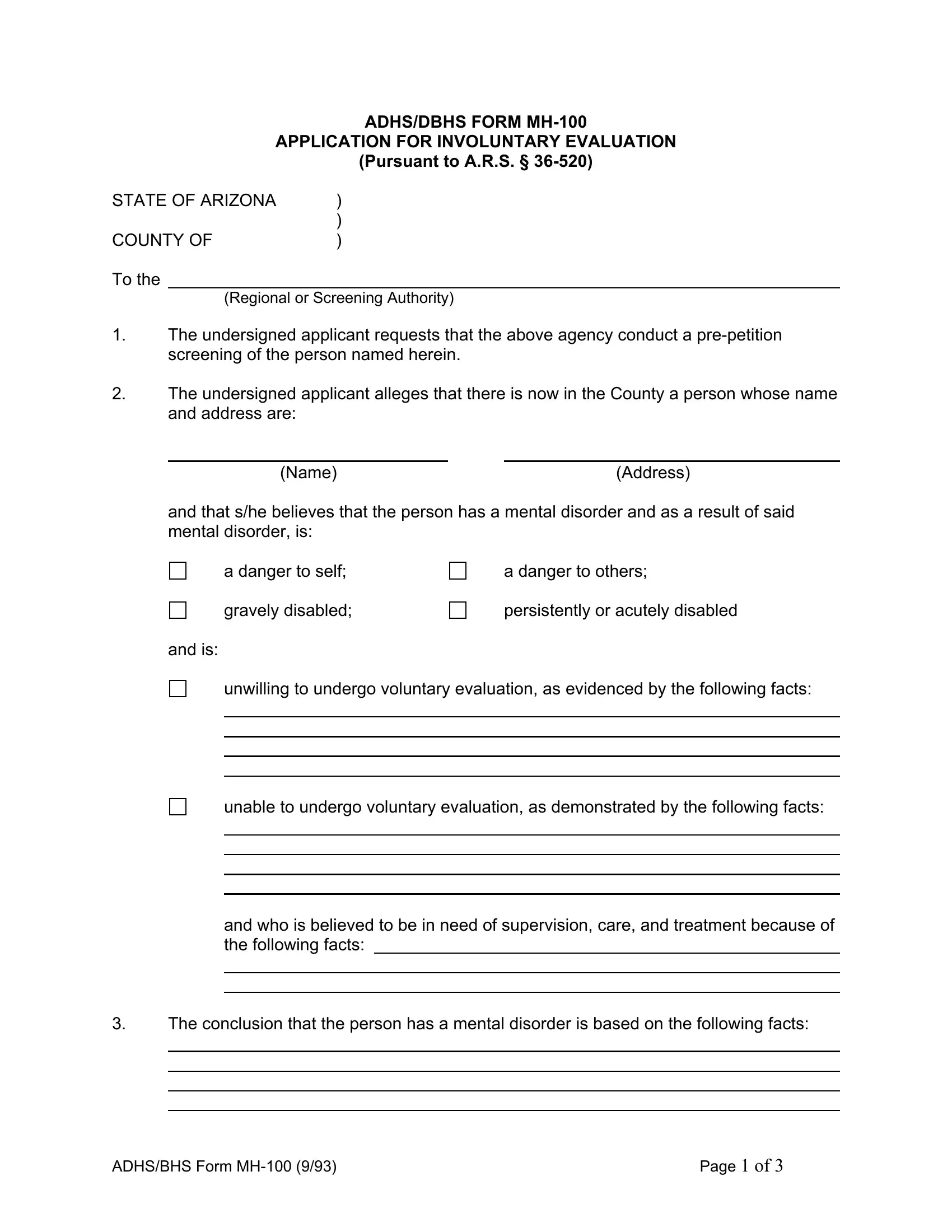
In the realm of mental health care within Arizona, the ADHS/DBHS Form MH-100 plays a pivotal role, serving as the Application for Involuntary Evaluation. It operates under the legal framework established by A.R.S. § 36-520, allowing concerned individuals to request that a person showing signs of a mental disorder undergo a pre-petition screening. The importance of this document can hardly be overestimated as it blends legal procedure with mental health intervention, aiming to ensure the safety and well-being of individuals who are believed to be a danger to themselves or others, or those who are gravely or persistently disabled. The form meticulously captures vital information ranging from personal data about the proposed patient—such as age, date of birth, sex, race, and more—to the specific reasons the applicant believes the individual requires involuntary evaluation. With the proper completion and submission of this form, it sets into motion a process that could lead to necessary medical intervention, potentially saving lives. Further cemented by the requirement of a notary public's certification, the formal procedure underscores the seriousness and sensitivity with which such cases are treated, ensuring a balance between the rights of the individual and the need for public safety.
| Question | Answer |
|---|---|
| Form Name | Adhs Bhs Form Mh100 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | arizona involuntary evaluation, arizona dbhs form online, arizona dbhs application, az dbhs form |
ADHS/DBHS FORM
APPLICATION FOR INVOLUNTARY EVALUATION
(PURSUANT TO A.R.S. §
STATE OF ARIZONA |
) |
|
) |
COUNTY OF |
) |
To the
(Regional or Screening Authority)
1.The undersigned applicant requests that the above agency conduct a
2.The undersigned applicant alleges that there is now in the County a person whose name and address are:
(Name) |
(Address) |
and that s/he believes that the person has a mental disorder and as a result of said mental disorder, is:
a danger to self;
a danger to others;
gravely disabled;
persistently or acutely disabled
and is:
unwilling to undergo voluntary evaluation, as evidenced by the following facts:
unable to undergo voluntary evaluation, as demonstrated by the following facts:
and who is believed to be in need of supervision, care, and treatment because of the following facts:
3.The conclusion that the person has a mental disorder is based on the following facts:
ADHS/BHS Form |
Page 1 OF 3 |
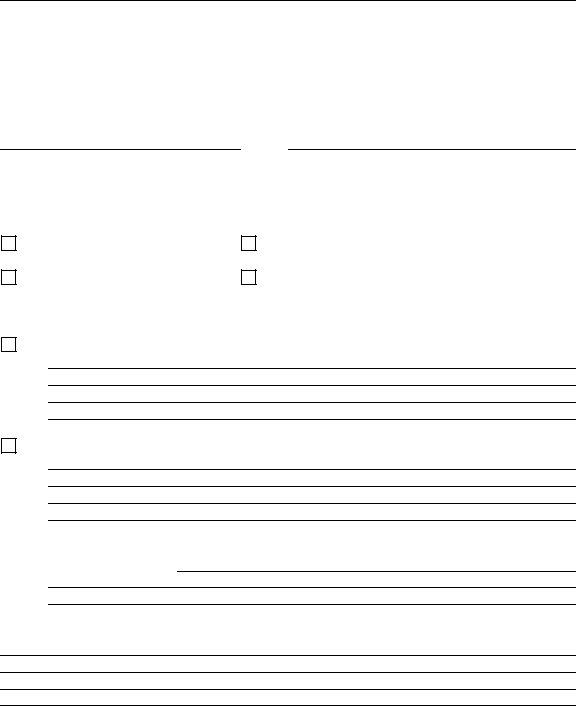
4.The conclusion that the person is dangerous or disabled is based on the following facts:
|
|
|
|
|
|
|
|
|
|
PERSONAL DATA OF PROPOSED PATIENT: |
|||||||||||||||||
Age |
|
|
Date of Birth |
|
|
Sex |
|
Race |
|
||||||||||||||||||
Weight |
|
|
|
|
Height |
|
|
Hair Color |
|
|
|
|
|
Eye Color |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Marital Status |
|
|
|
|
|
|
|
|
Number of Children |
|
|||||||||||||||||
Social Security No. |
|
|
Religion |
|
|
|
|
|
|
|
|
||||||||||||||||
Distinguishing Marks |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
Occupation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Present Location |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Dates and Places of Previous Hospitalization |
|
|
|
|
|
|
|
|
|||||||||||||||||||
How Long in Arizona |
|
|
State Last From |
|
|||||||||||||||||||||||
Veteran |
|
|
|
|
|
|
|
|
|
|
Education |
|
|||||||||||||||
NAME, ADDRESS AND TELEPHONE NUMBER OF:
1)Guardian
2)Spouse
3)Next of Kin
4)Significant Other Persons
DATE |
SIGNATURE OF APPLICANT |
|||
Printed or Typed Name of Applicant |
|
|||
Relationship to Proposed Patient |
|
|
||
Applicant’s Address |
|
|
||
Applicant’s Telephone |
|
|
||
ADHS/BHS Form |
Page 2 OF 3 |
SUBSCRIBED AND SWORN to before me this |
|
day of |
|
, 20 |
Notary Public
My Commission Expires:
ADHS/BHS Form |
Page 3 OF 3 |