
Filling out AF Form 4321 online is straightforward with FormsPal's free PDF editor. This guide covers each section of the Reserve Component Health Risk Assessment (RCHRA) so you can complete it accurately.
Step 1: Click "Get Form" at the top of this page to open the AF Form 4321 in our free online editor. No software installation is required.
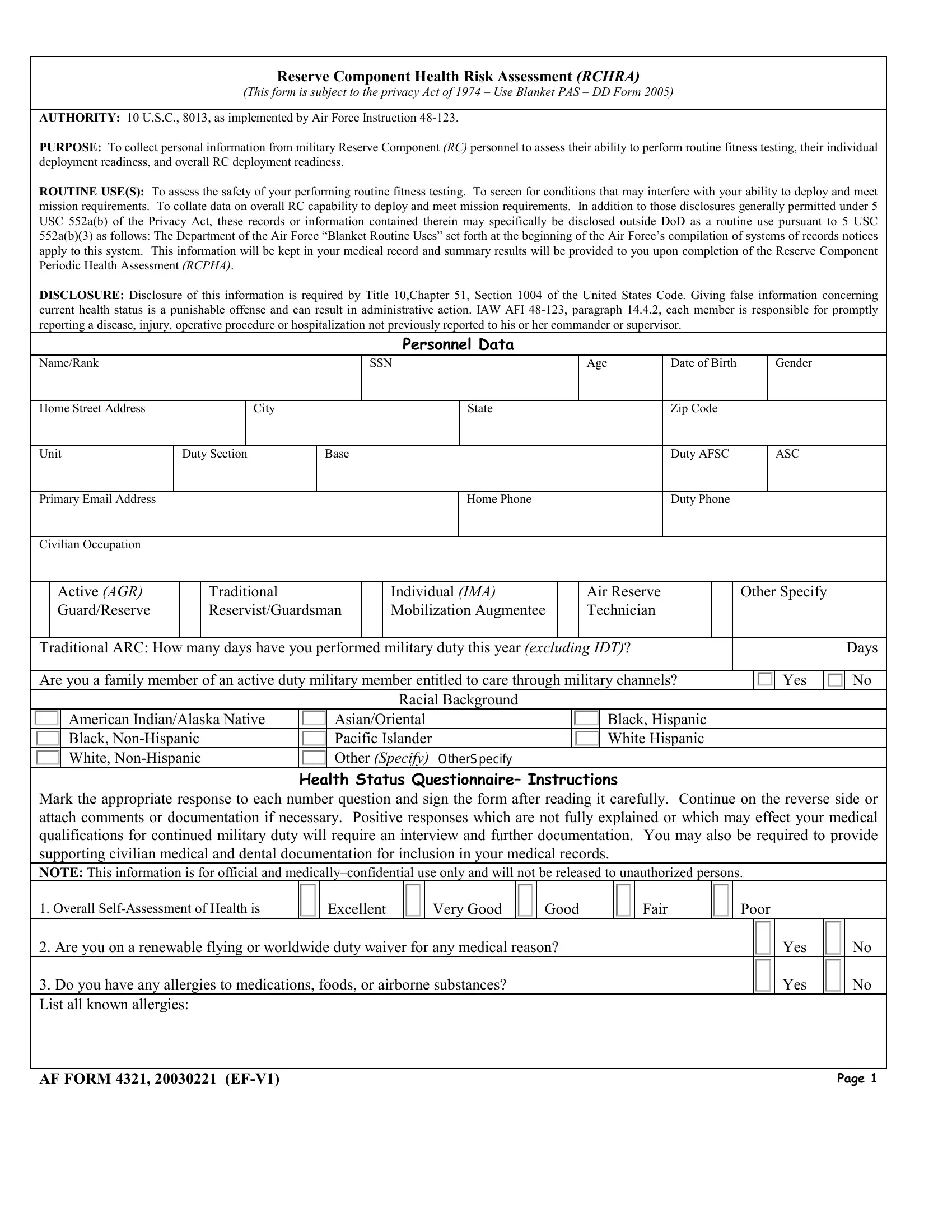
Step 2: Enter your overall health self-assessment rating (Excellent, Very Good, Good, Fair, or Poor). Answer yes or no for questions about renewable flying status and known allergies. Indicate whether you are on any current active duty orders.
Step 3: Complete the medications and health conditions section. List all prescription and over-the-counter medications you take regularly. Answer yes or no for each listed condition, including chest pain, shortness of breath, anxiety or depression, inflammatory bowel disease, and seizure disorder.
Step 4: Report your cardiovascular and general medical history. Include prior heart operations, family history of heart disease, high blood pressure diagnosis and treatment type (insulin, diet and exercise, or oral medication), and current tobacco and alcohol use habits.
Step 5: Complete the final section with your date, Name, Rank, and Social Security Number. Indicate your regular exercise program level (light, moderate, or heavy). Answer questions about physical limitations, bone or joint conditions, and any medications prescribed by a treating physician.
After reviewing all entries, click "Done" to finalize your AF Form 4321. FormsPal uses a secure system that never stores or shares your personal health information. Download the completed form and submit it to your unit health monitor or medical records office.
Common Questions About AF Form 4321
Who needs to fill out AF Form 4321? All Air Force Reserve Component members must complete this health risk assessment before fitness testing or deployment activities.
What authority requires AF Form 4321? The form is mandated under 10 U.S.C. 8013, implemented by Air Force Instruction 48-123, and protected by the Privacy Act of 1974.
What happens after submitting the form? Your unit health monitor reviews the completed RCHRA. Members reporting disqualifying conditions are referred to the base medical facility for a more detailed evaluation.
Related military health forms: Health Risk Assessment Form, AF Form 1288 (Ready Reserve Assignment), Air Force Form 1168, and FORSCOM Soldier Risk Assessment.