
aflac short term disability claim form 2021 can be filled out without difficulty. Simply use FormsPal PDF editor to complete the task fast. To keep our editor on the leading edge of convenience, we work to adopt user-driven capabilities and improvements regularly. We are routinely pleased to receive suggestions - help us with reshaping how we work with PDF documents. This is what you would need to do to get going:
Step 1: Just hit the "Get Form Button" in the top section of this page to open our pdf editor. There you'll find everything that is required to fill out your file.
Step 2: This tool enables you to customize PDF forms in various ways. Enhance it with customized text, correct what is originally in the document, and place in a signature - all at your fingertips!
With regards to the blank fields of this precise document, here is what you should know:
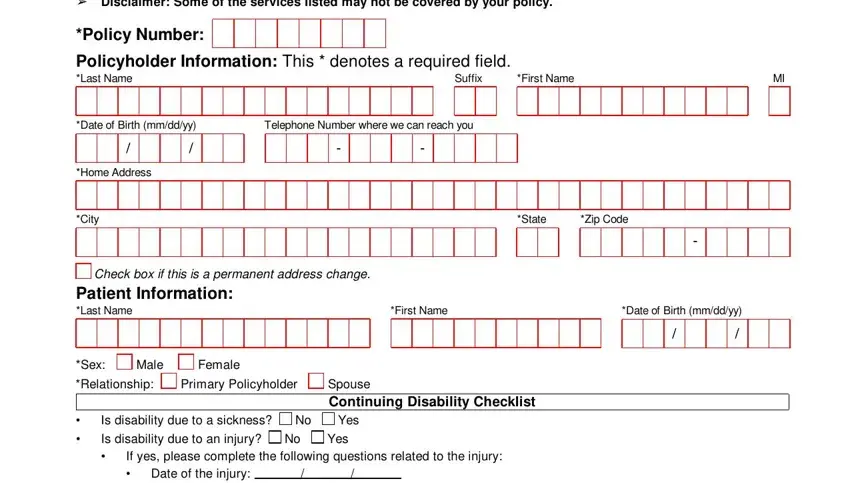
1. Complete your aflac short term disability claim form 2021 with a selection of major blanks. Gather all of the information you need and make certain there is nothing left out!
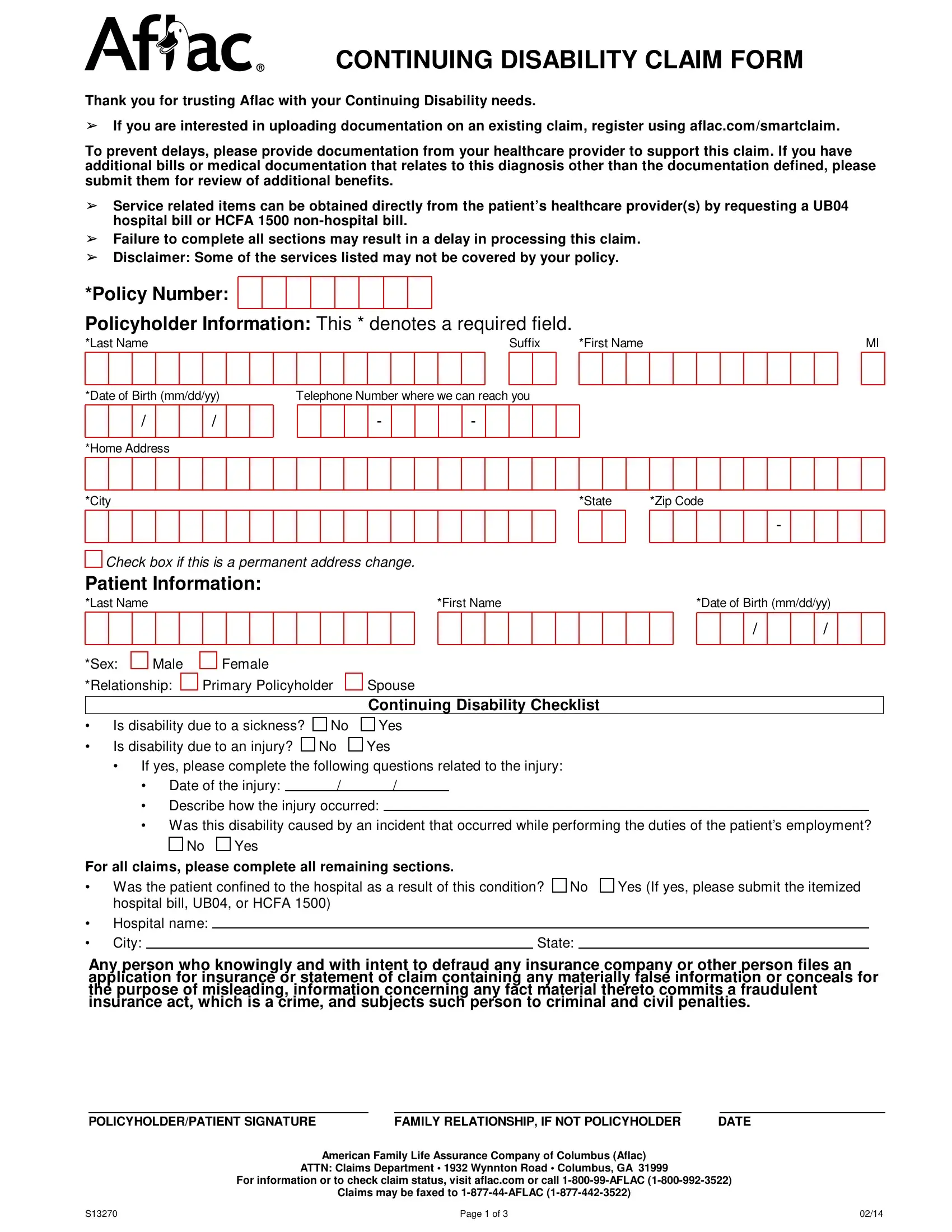
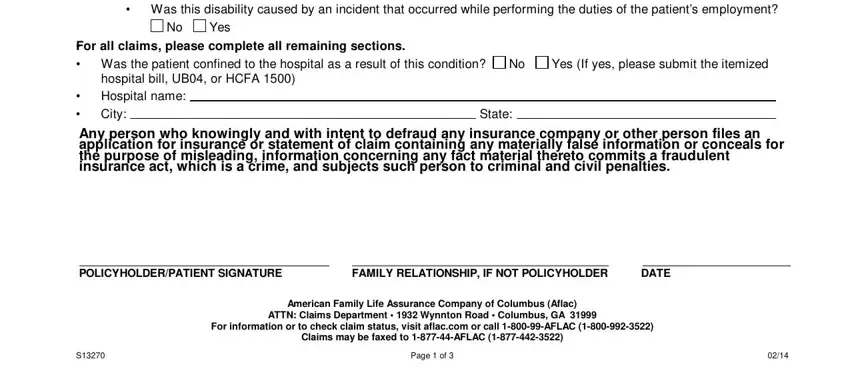
2. After this segment is done, you're ready insert the essential particulars in If yes please complete the, Yes, For all claims please complete all, Was the patient confined to the, Yes If yes please submit the, hospital bill UB or HCFA Hospital, State, Any person who knowingly and with, POLICYHOLDERPATIENT SIGNATURE, FAMILY RELATIONSHIP IF NOT, DATE, American Family Life Assurance, ATTN Claims Department Wynnton, For information or to check claim, and Claims may be faxed to AFLAC in order to go further.
3. The third part is generally easy - complete all of the blanks in CONTINUING DISABILITY CLAIM FORM , Policy Number, Policyholder Information This , Last Name, Suffix, First Name, Date of Birth mmddyy, Employees Name Last Name Suffix, Employers NameAccount , Employers Address, Employer Phone Number, State, Zip Code, City, and First date of disability to finish this process.
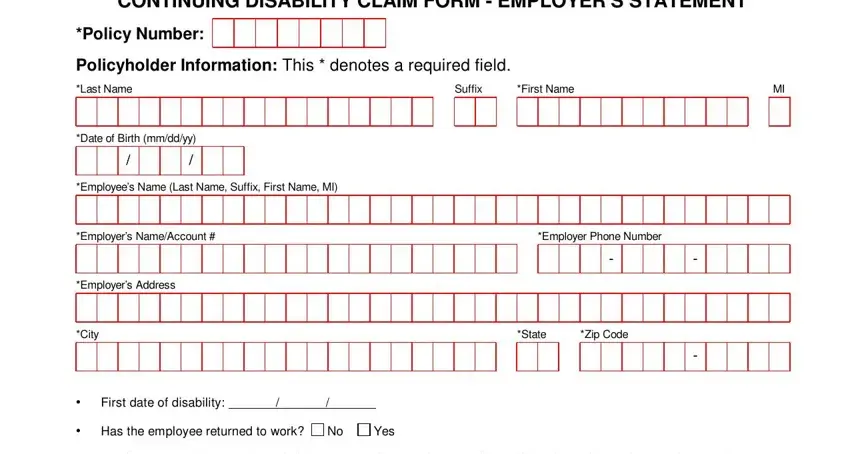
Be very careful when filling out Last Name and State, since this is where many people make errors.
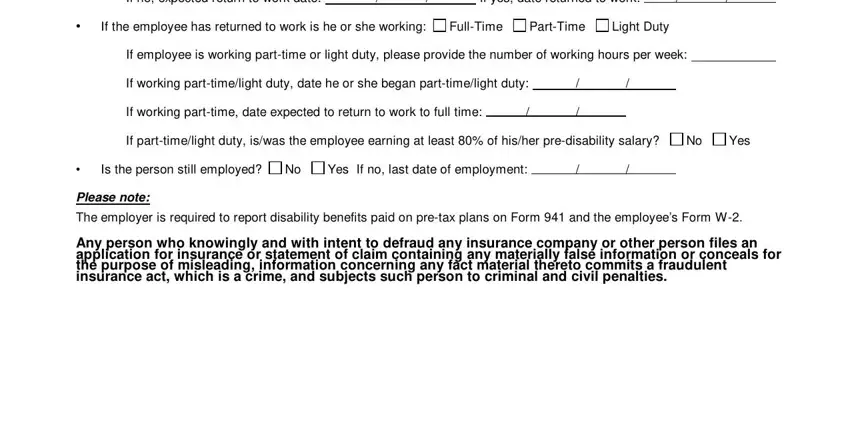
4. All set to fill in this next form section! In this case you will get all of these If no expected return to work date, If yes date returned to work, If the employee has returned to, FullTime, PartTime, Light Duty, If employee is working parttime or, If working parttimelight duty date, If working parttime date expected, If parttimelight duty iswas the, Yes, Is the person still employed, Yes If no last date of employment, Please note, and The employer is required to report blanks to fill out.
5. To conclude your form, this particular segment involves several extra blanks. Completing EMPLOYERS SIGNATURE, EMPLOYERS PRINTED NAME, TITLE, DIRECT PHONE NUMBER, DATE, American Family Life Assurance, ATTN Claims Department Wynnton, For information or to check claim, Claims may be faxed to AFLAC , and Page of should finalize the process and you will be done in a short time!

Step 3: After you've reviewed the information in the file's blank fields, simply click "Done" to finalize your document generation. Right after starting a7-day free trial account here, it will be possible to download aflac short term disability claim form 2021 or send it via email directly. The file will also be at your disposal in your personal account page with your each and every edit. FormsPal offers risk-free document completion with no personal information record-keeping or sharing. Feel safe knowing that your information is in good hands here!