
Once you open the online tool for PDF editing by FormsPal, it is easy to fill in or edit customerservicegmmusa right here. In order to make our editor better and easier to utilize, we continuously design new features, bearing in mind feedback coming from our users. With a few easy steps, you'll be able to begin your PDF editing:
Step 1: Press the orange "Get Form" button above. It'll open up our editor so you can start completing your form.
Step 2: After you open the file editor, you will find the form prepared to be filled out. Aside from filling out various blanks, it's also possible to perform many other actions with the Document, such as adding your own words, editing the initial text, adding graphics, affixing your signature to the document, and much more.
As for the blank fields of this particular form, this is what you should know:
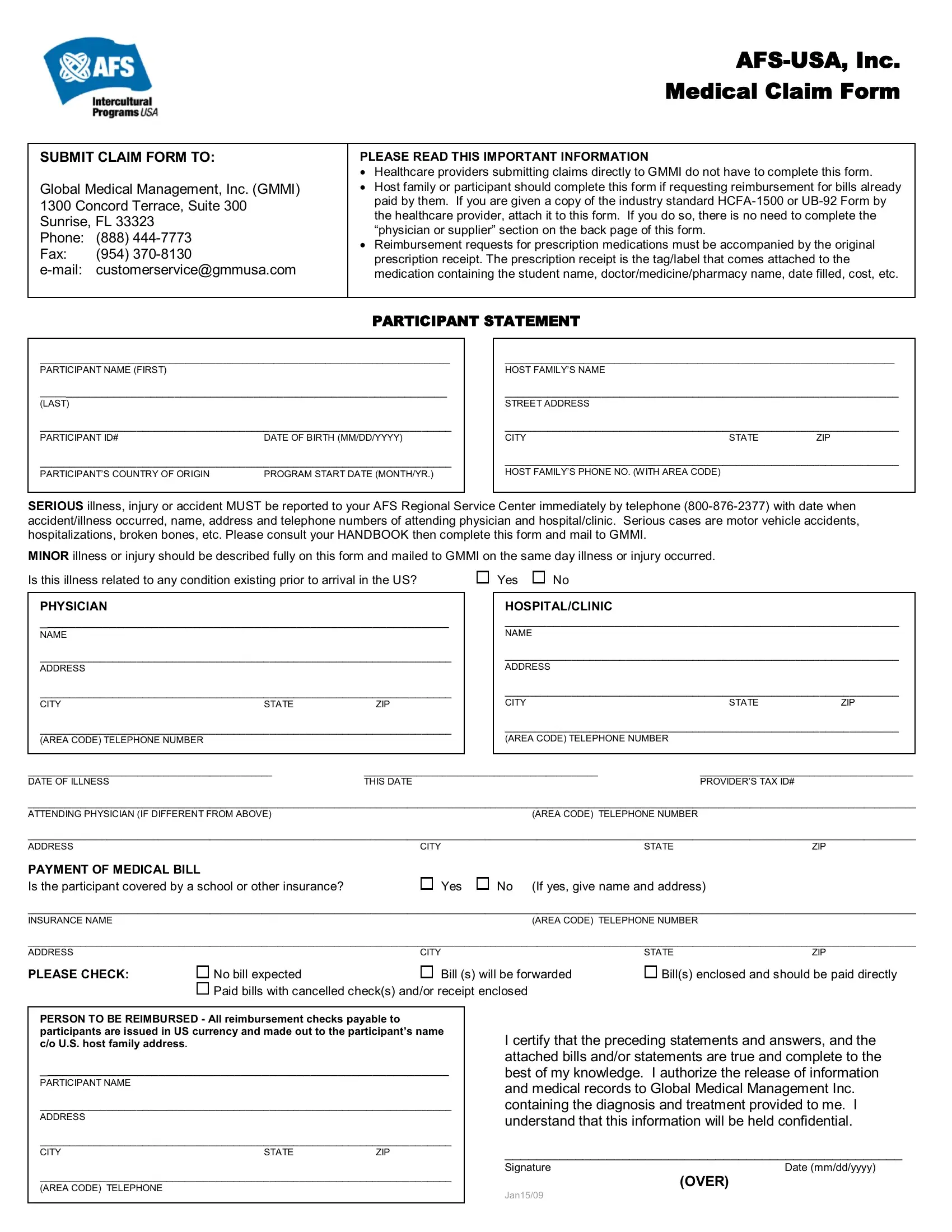
1. Start completing the customerservicegmmusa with a group of major blanks. Note all of the necessary information and be sure absolutely nothing is neglected!
2. Your next step would be to fill out the next few blank fields: PHYSICIAN NAME ADDRESS CITY , SERIOUS illness injury or accident, HOSPITALCLINIC NAME ADDRESS , No bill expected Paid bills with, THIS DATE, PROVIDERS TAX ID, Bills enclosed and should be paid, If yes give name and address, Bill s will be forwarded, AREA CODE TELEPHONE NUMBER, AREA CODE TELEPHONE NUMBER, Yes, STATE, STATE, and CITY.
As for If yes give name and address and HOSPITALCLINIC NAME ADDRESS , be certain that you take a second look in this current part. The two of these are thought to be the most important fields in the PDF.
3. In this step, examine DATE OF ACCIDENT, TIME OF ACCIDENT, ACCIDENT complete only if claim is, HOW DID THE ACCIDENT HAPPEN, WHERE DID THE ACCIDENT HAPPEN, NAME OF INSURANCE OF OTHER PARTIES, ADDRESS OF INSURANCE OF OTHER, TO HOSPITALS Attach to this form, PHYSICIANS AND SUPPLIERS If your, PHYSICIAN OR SUPPLIER INFORMATION, Date of ILLNESS first symptom or, Date patient first consulted you, Has patient ever had same or, Yes, and Please check If other than. Every one of these will have to be filled in with greatest focus on detail.
4. The following section needs your information in the following places: DIAGNOSES May use ICDCM or DSM III, PRIMARY SECONDARY, Date of Service, Place of Service, Procedure Codes Identify, Full describe procedures types of, Charges, Amount Paid, Balance Due, SIGNATURE OF PROVIDER DATE DEGREE, Total Charge, Amount Paid, Balance Due, YOUR PATIENTS ACCOUNT NUMBER, and ADDRESS CITY STATE ZIP. Ensure that you type in all required info to go further.
5. This last section to conclude this PDF form is crucial. Ensure to fill in the necessary blank fields, and this includes ADDRESS OF ATTENDING PHYSICIAN, ATTENDING PHYSICIANS SIGNATURE, Place of service codes, H, Inpatient Hospital, OH, Outpatient Hospital, O, Doctors Office, Patients Home, Day Care Facility Psy, Night Care Facility Psy, NH, Nursing Home, and SNF, prior to finalizing. Otherwise, it might contribute to a flawed and probably incorrect document!
Step 3: Just after proofreading the form fields you've filled out, hit "Done" and you're done and dusted! Sign up with us right now and easily obtain customerservicegmmusa, available for downloading. Every last edit made is conveniently preserved , helping you to customize the file later on as needed. FormsPal ensures your data confidentiality with a protected system that never records or shares any kind of private information used. Rest assured knowing your documents are kept protected whenever you work with our service!