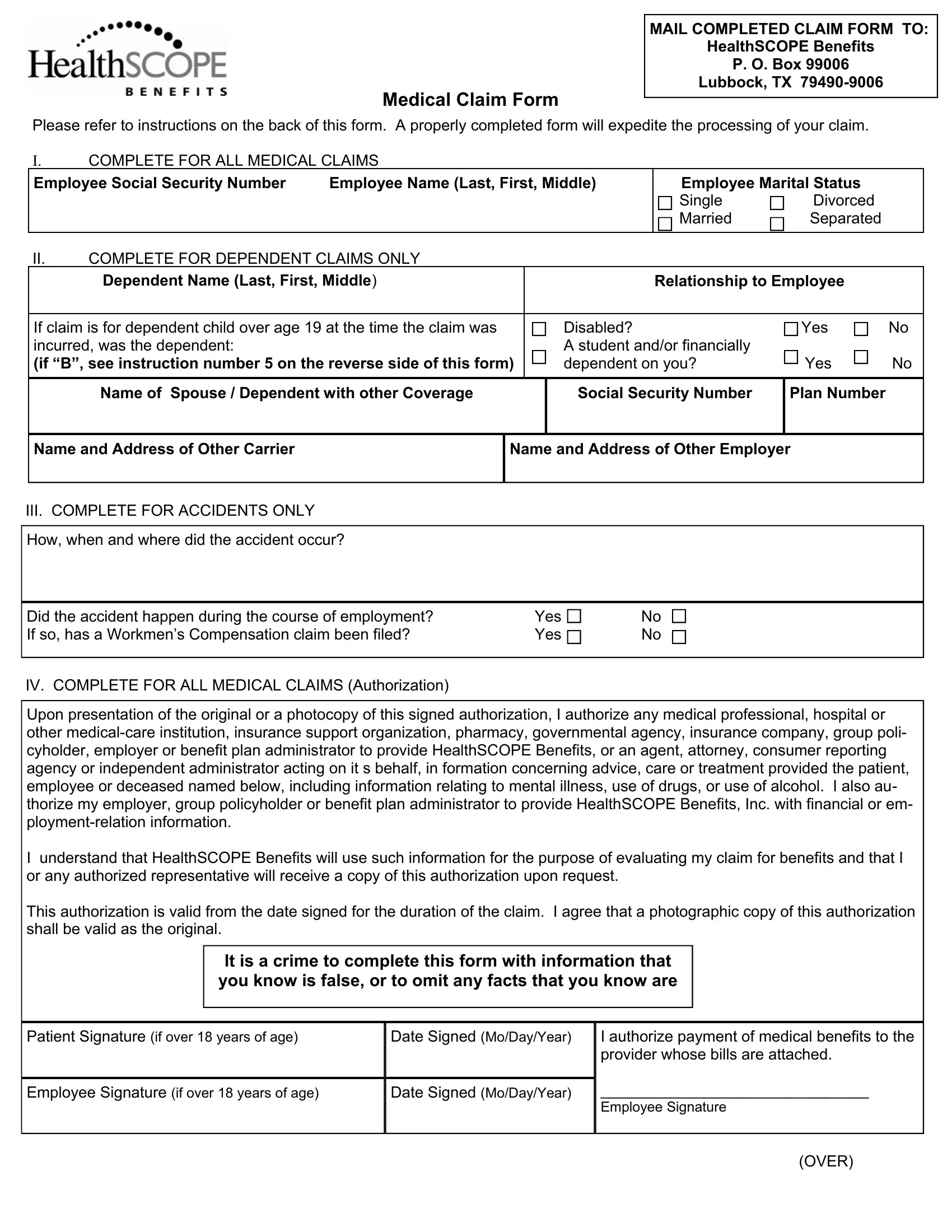
In today's healthcare landscape, navigating the intricacies of medical claim forms is paramount for the timely and efficient processing of healthcare benefits. Among these, the Healthscope Medical Claim Form stands as a critical document designed to streamline the reimbursement process for medical services rendered. Tailored to facilitate the submission of claims, this form requires comprehensive details covering all aspects of medical services—ranging from personal identification to specific information concerning the nature of medical treatments or accidents. By submitting the claim to HealthSCOPE Benefits at the provided address, individuals ensure that their claims are processed efficiently. The form underscores the necessity for meticulous completion, including the requirement of itemized bills and, if applicable, an Explanation of Benefits (EOB) from primary carriers. Furthermore, it accommodates different scenarios, such as claims for dependents, accidents, and instances necessitating authorization for the release of medical or employment-related information, highlighting the form’s versatility in addressing varied healthcare claims. The act of signing the form manifests the claimant's acknowledgment of its accuracy and grants permission for HealthSCOPE Benefits to access needed information to evaluate the claim. It underscores the form's central role in the claims process, facilitating communication between patients, healthcare providers, and insurance administrators to ensure that claims are resolved in a timely manner.
| Question | Answer |
|---|---|
| Form Name | Healthscope Medical Claim Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 9 |
| Avg. time to fill out | 2 min 18 sec |
| Other names | policyholder, Workmens, payor, Lubbock |