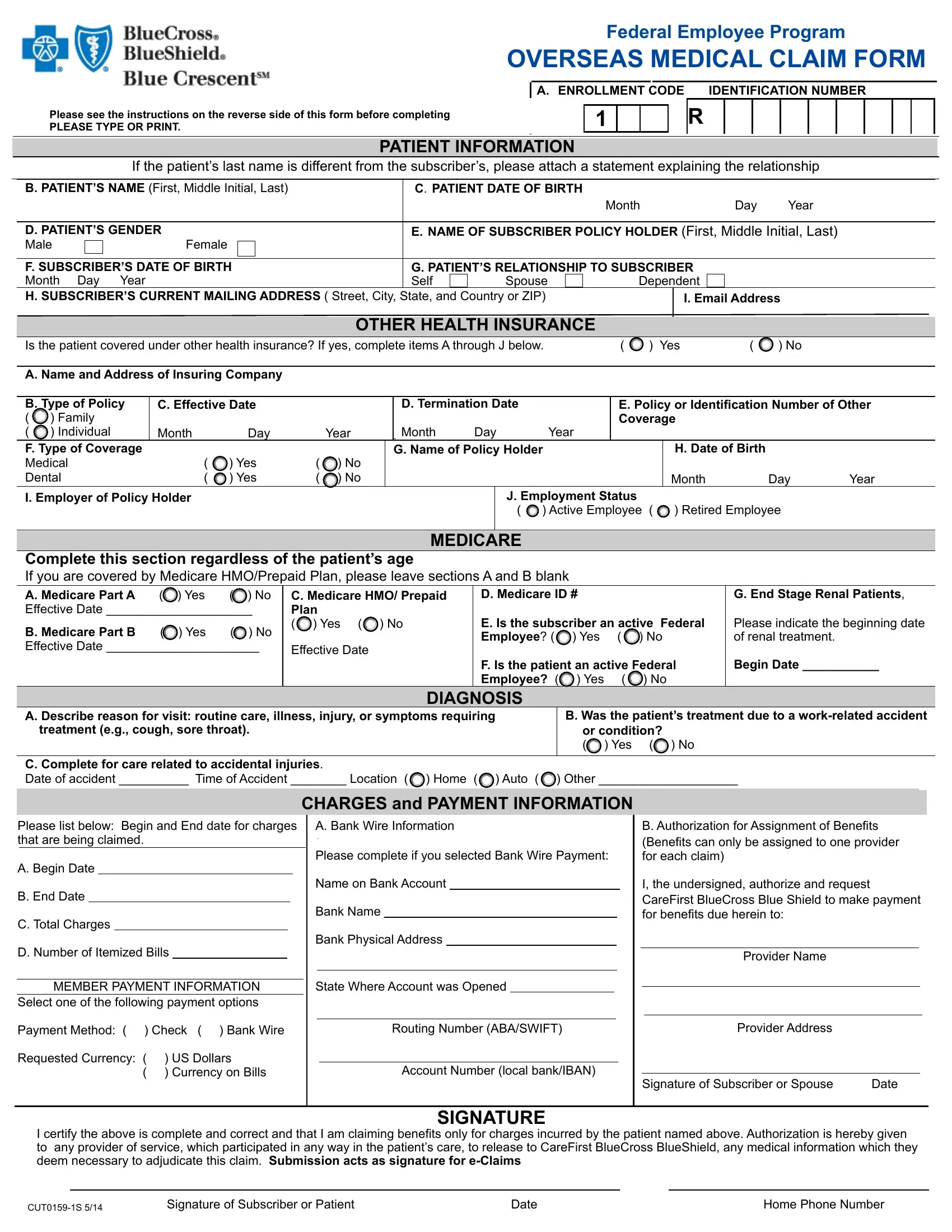
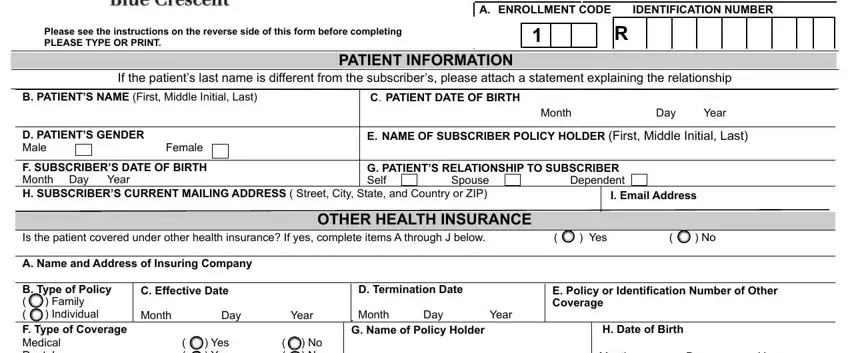
FEDERAL EMPLOYEE PROGRAM OVERSEAS MEDICAL CLAIM FORM
PLEASE USE THE RETAIL PRESCRIPTION DRUG OVERSEAS CLAIM FORM FOR ALL PRESCRIPTION DRUGS PURCHASED AT PHARMACIES OUTSIDE OF THE UNITED STATES, PUERTO RICO, AND THE U.S. VIRGIN ISLANDS
GENERAL INFORMATION
This Overseas Medical Claim Form is to be used to submit a claim for beneits for covered services received outside the United States, Puerto Rico, and the U.S. Virgin Islands. Please complete a separate claim form for each patient and remember to ile all claims by December 31 of
the calendar year after the one in which the covered care or service was provided.
The Overseas Medical Claim Form must be completed in full, and accompanied by fully itemized bills. Please be sure to keep photocopies of
all bills and supporting documentation for your personal records.
ITEMIZED BILL INFORMATION
Each provider’s original itemized bill must be attached and must contain:
–The letterhead indicating the name and address of the person or organization providing the service
–The full name of the patient receiving the service
–The date of each service
–A description of each service
–The charge for each service
OVERSEAS MEDICAL CLAIM FORM INSTRUCTIONS
Please complete all items on the claim form. If the information requested does not apply to the patient, indicate N/A (Not Applicable). Special care should be taken when completing the following items:
OTHER HEALTH INSURANCE – If the patient holds other insurance coverage, please complete items A through J as completely as possible. It is especially important to indicate the name and address of the other insurance company and the policy or identiication number of that
coverage, as well as the name and birth date of the person who holds that policy.
In addition, if the patient is someone other than the Policy Holder and has received beneits from any other health insurance plan held by reason of law or employment, the Explanation of Beneits Form furnished by the other carrier pertaining to these charges must be included with the claim.
A clear photocopy of the other carrier’s Explanation of Beneits Form is acceptable in place of the original document.
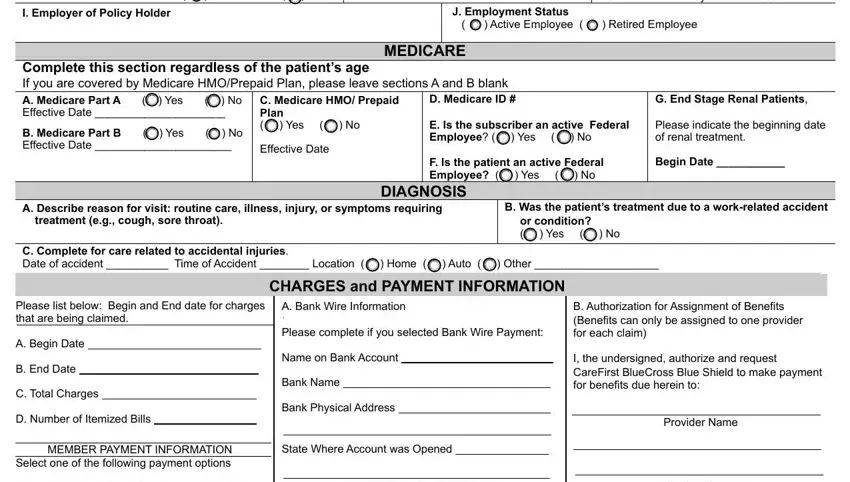
MEDICARE – Medicare beneits are often limited for care provided outside the United States and its territories. Please refer to your Medicare handbook. However, please complete item 3 regardless of the patient’s age.
DIAGNOSIS – Describe reason for visit, illness, injury, or symptoms requiring treatment, e.g. cough, sore throat.
CHARGES – Please list here the number of bills that are being included on this claim. Please attach itemized bills for all services. Please list the beginning date and the end date of service.
A.Begin Date- The irst date of service for which beneits are being claimed
B.End Date- The last date of service for which beneits are being claimed
C.Total Charges- The total amount being claimed for all bills attached.
D.Number of Itemized Bills Attached- Total number of itemized bills for all services being claimed.
MEMBER PAYMENT INFORMATION – Make payment to subscriber, designation of currency and payment method – Indicate whether you want to be paid in the currency relected on the bill(s) or in U.S. dollars and if you want to receive payment via check or bank wire. Please
note that not all forms of currency may be available for payment. In the event that you select payment in a currency that is not available, you will be paid in U.S. dollars. Banks will typically charge a lat fee or percentage-based fee to receive a wire. You may want to investigate fees
charged by your bank prior to requesting a wire since you will be responsible for any such fees.
BANK WIRE INFORMATION – You must include the following information on this form: your full name (initials are not acceptable) and your physical address (payments cannot be sent to a P.O. Box). For wire payments, subscriber’s name as it appears on the bank account, the bank’s name and physical address (payments cannot be wired to a P.O. Box), account number, ABA number. Please provide a copy of a
voided check or deposit slip so that the bank information can be validated. Additionally, for wire payments to European Union countries, you must provide the International Bank Account Number (IBAN) and Bank Identiier Code (ABA/SWIFT). For checks to be sent by express mail,
you must provide a current telephone number.
AUTHORIZATION FOR ASSIGNMENT OF BENEFITS – Complete this item if you prefer that beneits be paid directly to the provider of service.
SIGNATURE – The Overseas Medical Claim Form must be signed and dated by the Policy Holder, spouse, or the patient.
Submission acts as signature for e-Claims
THIS COMPLETED CLAIM FORM, TOGETHER WITH ITEMIZED BILLS AND SUPPORTING DOCUMENTATION, SHOULD BE SUBMITTED TO:
Federal Employee Program (FEP) Overseas Claims, PO Box 261570, Miami, FL 33126 YOU CAN ALSO FAX YOUR CLAIMS TO EITHER 1-888-650-6525 OR 410-781-7637
DEPENDING ON THE LOCATION THAT YOU FAX FROM, YOU MAY NOT NEED TO ADD THE 1 IN FRONT OF THE 888 FAX NUMBER.
ADDITIONAL CLAIM FORMS and FAX DIALING INSTRUCTIONS AVAILABLE ON www.fepblue.org. OR BY CALLING 1-888-999-9862