
fillable form 362 alabama medicaid referral can be filled in without difficulty. Simply make use of FormsPal PDF editing tool to accomplish the job quickly. In order to make our editor better and more convenient to use, we continuously work on new features, taking into account suggestions from our users. Getting underway is simple! Everything you need to do is take these basic steps down below:
Step 1: First of all, access the pdf editor by pressing the "Get Form Button" in the top section of this page.
Step 2: This editor will allow you to change the majority of PDF forms in various ways. Transform it with any text, adjust what's already in the PDF, and include a signature - all within several clicks!
This document will need specific data to be filled out, therefore be sure to take whatever time to provide exactly what is expected:
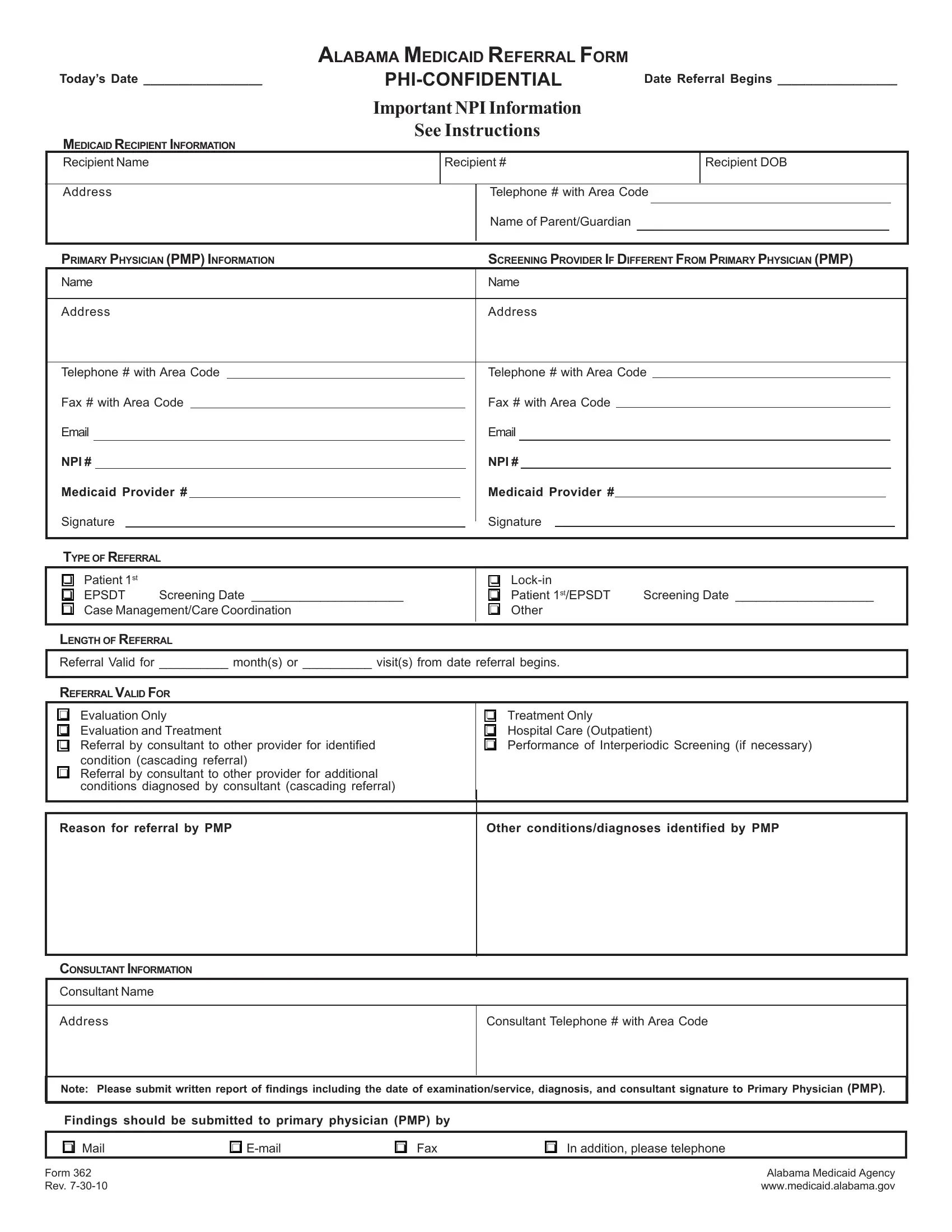
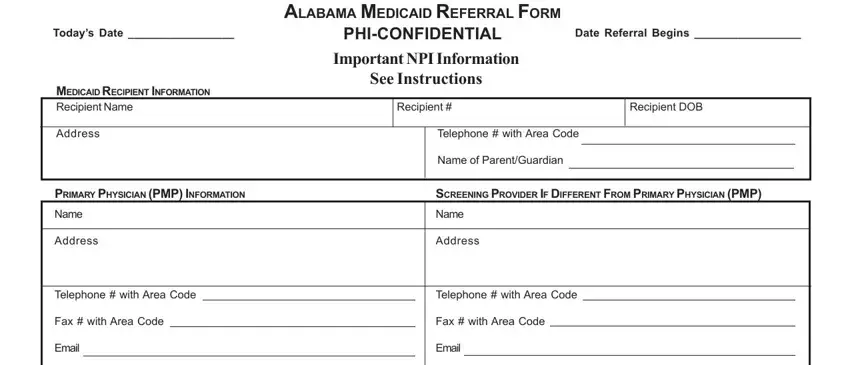
1. The fillable form 362 alabama medicaid referral needs specific information to be typed in. Ensure that the following blank fields are completed:
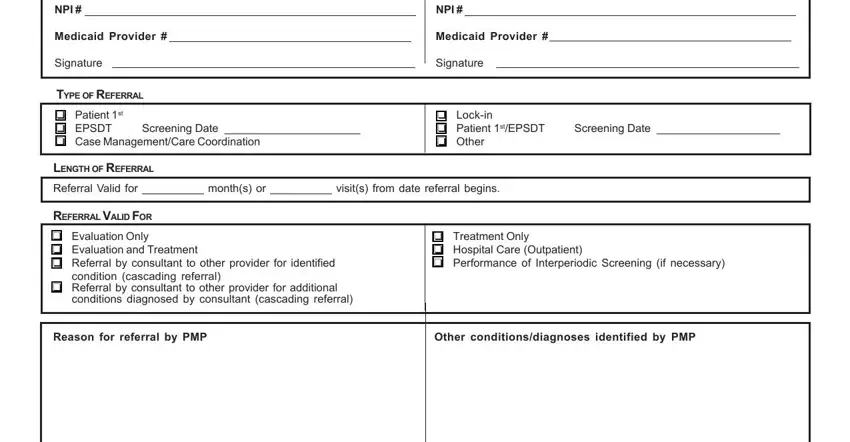
2. The subsequent step is usually to submit these particular fields: NPI , Medicaid Provider , Signature, TYPE OF REFERRAL, NPI , Medicaid Provider , Signature, Patient st EPSDT Screening Date , Lockin Patient stEPSDT Screening, LENGTH OF REFERRAL, Referral Valid for months or , REFERRAL VALID FOR, Evaluation Only Evaluation and, condition cascading referral, and Referral by consultant to other.
3. This next step is focused on CONSULTANT INFORMATION, Consultant Name, Address, Consultant Telephone with Area, Note Please submit written report, Findings should be submitted to, Mail, Form Rev , Email, Fax, In addition please telephone, and Alabama Medicaid Agency - complete all these blank fields.
As to In addition please telephone and CONSULTANT INFORMATION, be sure that you double-check them here. Both of these are certainly the key ones in this document.
Step 3: Ensure the details are accurate and click "Done" to progress further. Join FormsPal right now and instantly get fillable form 362 alabama medicaid referral, all set for download. All alterations made by you are saved , making it possible to edit the form at a later time if required. If you use FormsPal, you'll be able to fill out documents without having to get worried about database incidents or entries being distributed. Our secure platform ensures that your private data is stored safely.