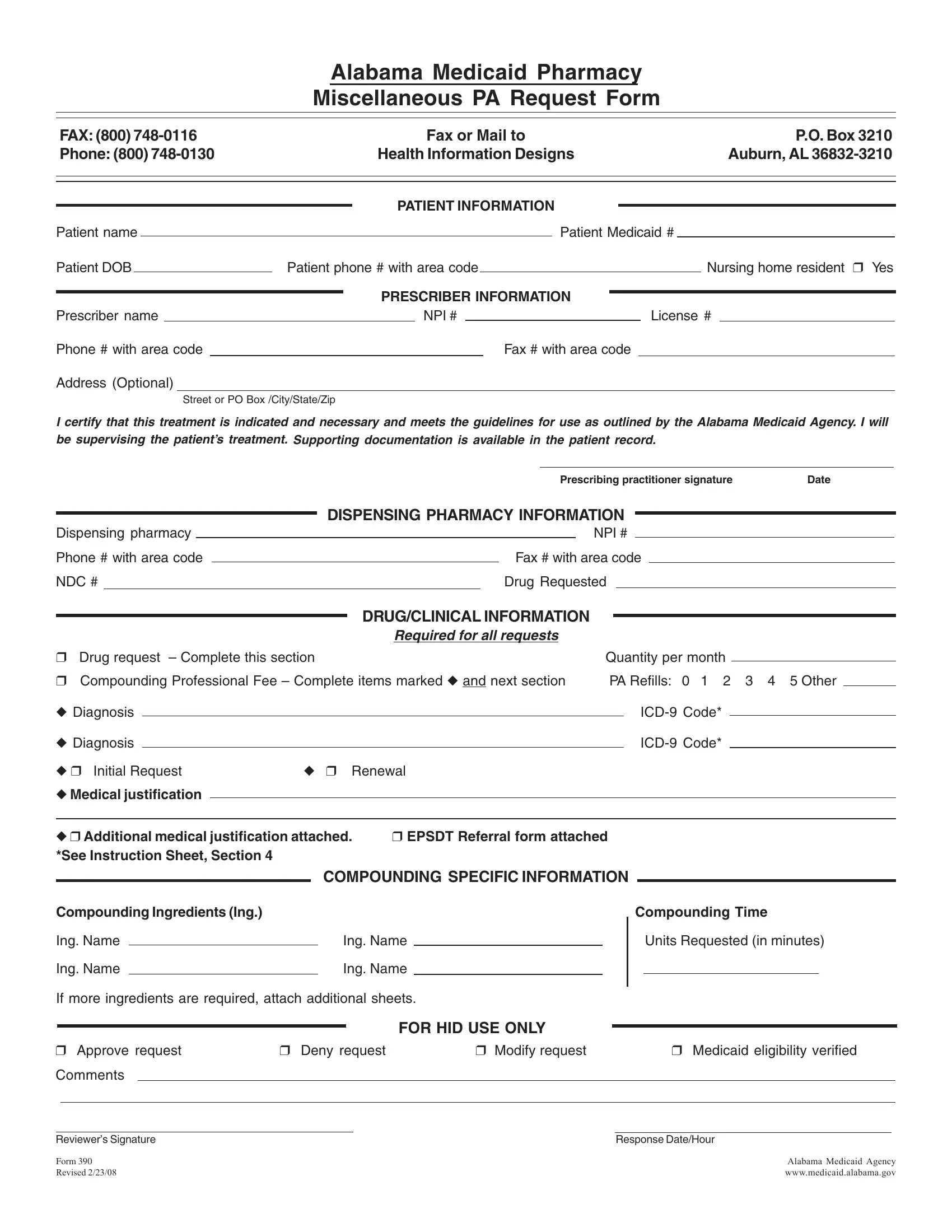
The Alabama 390 form serves a vital role within the healthcare system for Medicaid recipients, streamlining the process for pharmacists and prescribers to request prior authorization for miscellaneous pharmacy requests. This crucial document, designed to be sent to Health Information Designs via fax or mail, encompasses a wide range of information, including patient details such as name, Medicaid number, and date of birth, as well as prescriber and dispensing pharmacy information. The form requires comprehensive data including the National Provider Identifier (NPI) and license numbers of the prescriber, and specifics about the drug requested including diagnosis codes, quantity, and medical justifications for the treatment. It uniquely addresses scenarios involving compounding prescriptions by accommodating details about compounding ingredients and time units requested. Designed to ensure treatments meet Alabama Medicaid Agency guidelines, the form also facilitates support for treatments through the Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) service for eligible individuals. By mandating detailed substantiation for requested treatments, including a certification from the prescribing practitioner about the necessity and adherence to guidelines, the Alabama 390 form exemplifies a structured approach to healthcare provision for Medicaid enrollees, ensuring that only necessary and approved medications are dispensed.
| Question | Answer |
|---|---|
| Form Name | Alabama Form 390 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | NDC, DOB, alabama medicaid pa form, Reviewers |
Alabama Medicaid Pharmacy
Miscellaneous PA Request Form
FAX: (800) |
|
|
|
Fax or Mail to |
|
|
|
|
P.O. Box 3210 |
|||||||||||
Phone: (800) |
|
|
Health Information Designs |
|
|
|
|
Auburn, AL |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT INFORMATION |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Patient name |
|
|
|
|
|
|
|
|
Patient Medicaid # |
|
|
|
||||||||
Patient DOB |
|
Patient phone # with area code |
|
|
|
|
|
|
Nursing home resident ❒ Yes |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRESCRIBER INFORMATION |
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Prescriber name |
|
|
|
|
|
|
NPI # |
|
|
License # |
|
|||||||||
Phone # with area code |
|
|
|
|
|
|
|
Fax # with area code |
|
|
|
|
|
|||||||
Address (Optional) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Street or PO Box /City/State/Zip
I certify that this treatment is indicated and necessary and meets the guidelines for use as outlined by the Alabama Medicaid Agency. I will be supervising the patient’s treatment. Supporting documentation is available in the patient record.
Prescribing practitioner signature |
Date |
DISPENSING PHARMACY INFORMATION
Dispensing pharmacy Phone # with area code NDC #
NPI #
Fax # with area code Drug Requested
DRUG/CLINICAL INFORMATION
Required for all requests
❒ |
Drug request – Complete this section |
|
Quantity per month |
|
|
|||||
|
|
|
||||||||
❒ |
Compounding Professional Fee – Complete items marked ◆ and next section |
PA Refills: |
0 1 2 3 4 5 Other |
|
||||||
◆ Diagnosis |
|
|
|
|
Code* |
|
||||
|
|
|
|
|
||||||
◆ Diagnosis |
|
|
|
|
Code* |
|
||||
◆ ❒ Initial Request |
◆ |
❒ Renewal |
|
|
|
|
|
|
||
◆Medical justification
◆ ❒ Additional medical justification attached. |
❒ EPSDT Referral form attached |
*See Instruction Sheet, Section 4 |
|
COMPOUNDING SPECIFIC INFORMATION
Compounding Ingredients (Ing.) |
|
|
Ing. Name |
|
Ing. Name |
|
||
Ing. Name |
|
Ing. Name |
If more ingredients are required, attach additional sheets.
Compounding Time
Units Requested (in minutes)
FOR HID USE ONLY
❒ Approve request |
❒ Deny request |
❒ Modify request |
❒ Medicaid eligibility verified |
||||
Comments |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Reviewer’s Signature |
|
|
|
Response Date/Hour |
|||
FORM 390 |
|
|
|
Alabama Medicaid Agency |
|||
Revised 2/23/08 |
|
|
|
www.medicaid.alabama.gov |
|||