
 Readable PDF sent by secure email
Readable PDF sent by secure email
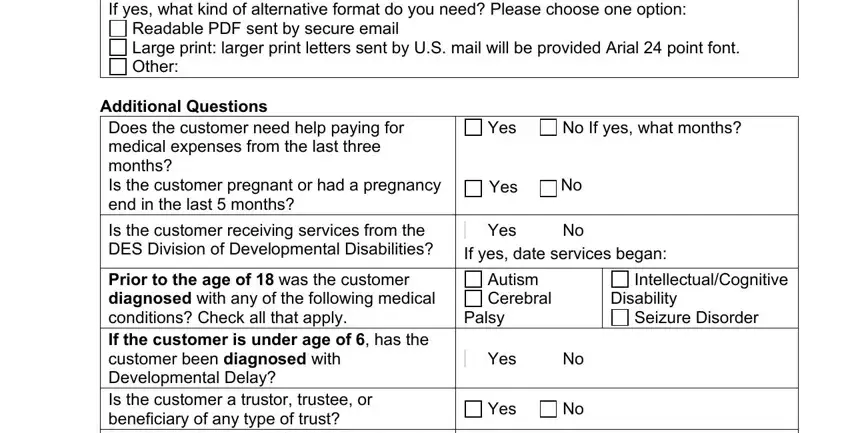
 Large print: larger print letters sent by U.S. mail will be provided Arial 24 point font.
Large print: larger print letters sent by U.S. mail will be provided Arial 24 point font.  Other:
Other:

 Customer
Customer
 Spouse of the customer
Spouse of the customer
 Parent of the customer (if the customer is a minor)
Parent of the customer (if the customer is a minor)

 I specifically authorize the holder of my information to disclose all of my educational and evaluation records in its possession to AHCCCS.
I specifically authorize the holder of my information to disclose all of my educational and evaluation records in its possession to AHCCCS.
Our PDF editor was made with the intention of allowing it to be as simple and intuitive as possible. These steps can certainly make filling out the altcs fast and simple.
Step 1: Look for the button "Get Form Here" on this webpage and click it.
Step 2: Now you may enhance the altcs. You can use our multifunctional toolbar to insert, erase, and modify the content material of the form.
Create the following areas to prepare the template:
Include the required information in the Divorced, Widowed Date of spouses death, Spouses Name Last First Middle, Spouses Date of Birth, Spouses Social Security Number, Customers Home Address, Customers Mailing Address if, Phone Number, EMail Address, Authorized RepresentativeSpouse, Name of the Customers Legal, Relationship to Customer, Authorized Representatives Mailing, City, and State section.
In the segment discussing City, State, Zip Code, Phone Number, EMail Address, DEDE Combo form, and Page of, it's important to jot down some demanded particulars.

The Legal GuardiansConservators, City, State, Zip Code, Phone Number, EMail Address, Customers Current Living, Hospital At Home, Nursing Facility Other, Date Admitted Expected Date of, Name of the Hospital Assisted, Phone Number, Hospital Assisted Living or, City, and State box is the place to insert the rights and responsibilities of both sides.
Finalize the document by looking at the following fields: If yes what kind of alternative, Readable PDF sent by secure email, Additional Questions Does the, Yes, No If yes what months, Yes, Is the customer receiving services, Yes, No If yes date services began, Prior to the age of was the, Autism Cerebral, Palsy, IntellectualCognitive, Disability, and Seizure Disorder.
Step 3: As soon as you are done, click the "Done" button to upload the PDF document.
Step 4: Produce copies of your form. This should protect you from possible issues. We do not read or display the information you have, as a consequence you can be confident it is protected.
