Use our free PDF editor to complete the ALTCS application online. Before starting, confirm basic eligibility: Arizona residency, age 65 or older (or qualifying disability), and need for nursing-level care.
Step 1: Click "Get Form Here" on this page to open the ALTCS application in the editor.
Step 2: Fill in your personal information using the toolbar to type or modify any field.
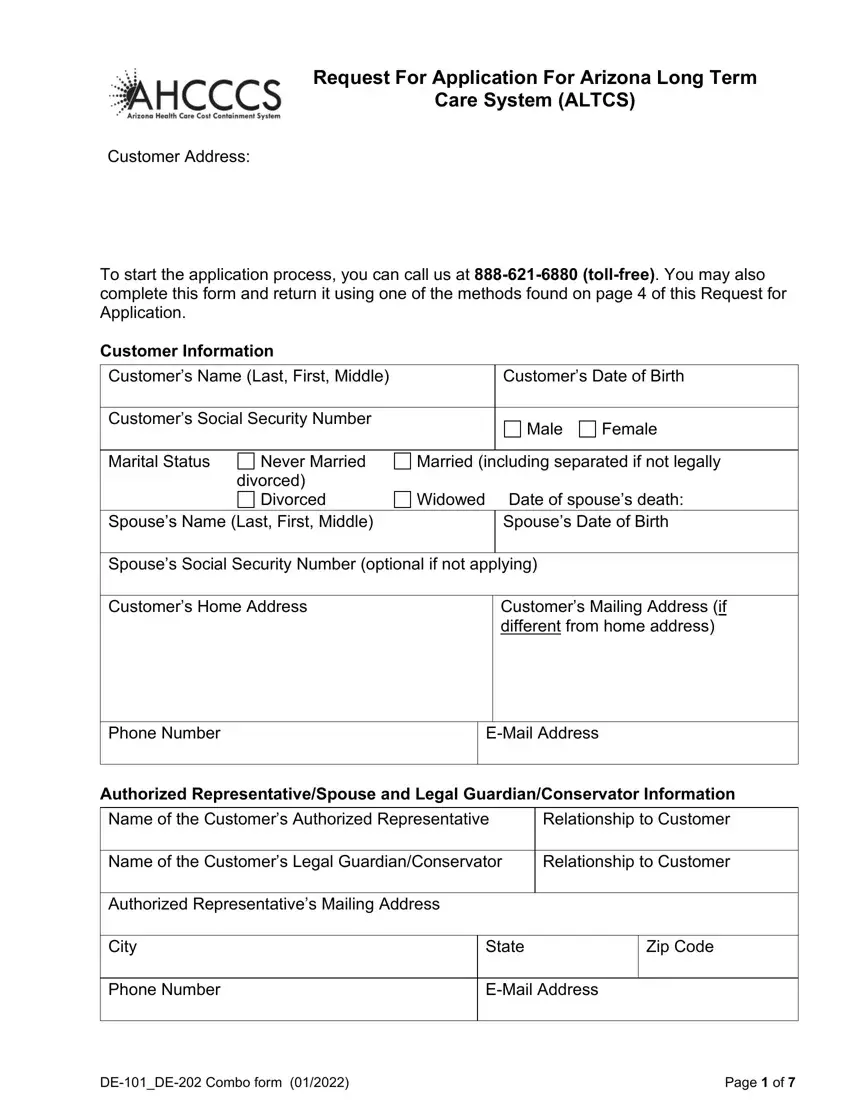
Complete the personal details section first:
Enter your name, date of birth, Social Security number, home address, mailing address, phone number, and email. Add your authorized representative or legal guardian information if applicable.
Fill in city, state, ZIP code, phone, and email in the next section. Complete the DEDE Combo form and page numbering fields.

Complete the legal guardian or conservator section with their contact details. Describe your current living situation: at home, in a hospital, assisted living, or nursing facility. Include the admission date and facility name if applicable.
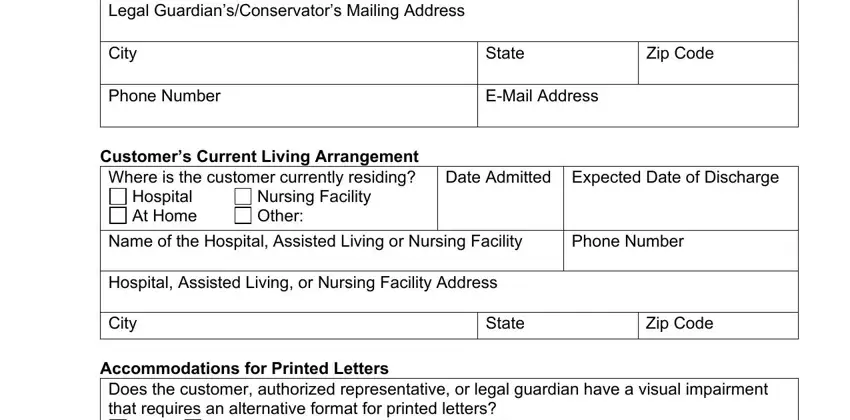
Answer the disability and diagnosis questions. Indicate conditions such as autism, cerebral palsy, intellectual disability, or seizure disorder. Note whether you already receive Medicaid services and the date services began.
Step 3: Click "Done" to download the completed ALTCS application PDF.
Step 4: Save copies for your records. Your information is encrypted and private. Submit to AHCCCS by phone, fax, email, or in person. For other care applications, see the KanCare Application.
