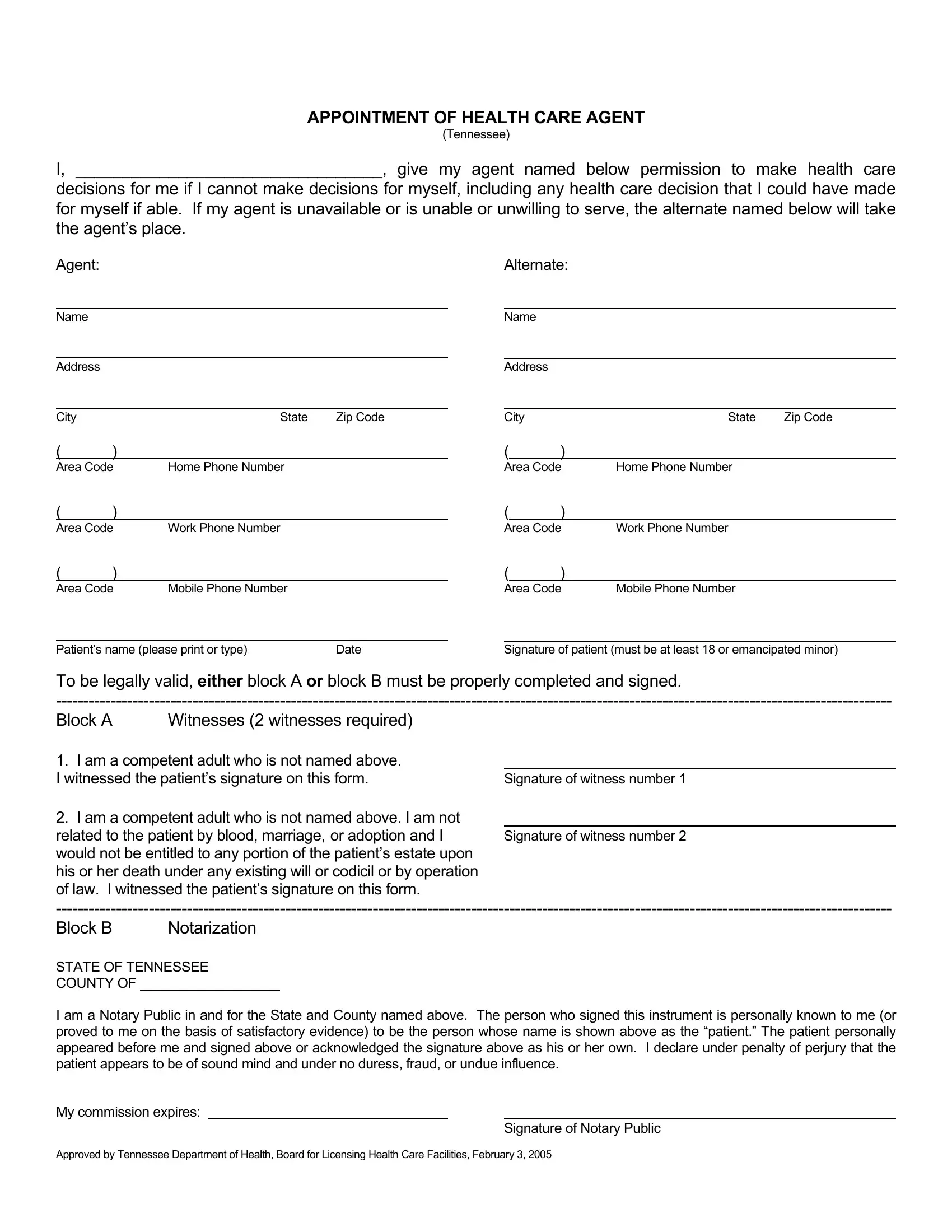
The Appointment of Health Care Agent form is a critical document allowing individuals to designate someone to make health care decisions on their behalf in the event they are unable to do so themselves. This comprehensive directive, specifically tailored for Tennessee residents, outlines the process for selecting a primary agent and an alternate to ensure decisions can be made even if the primary agent is unavailable, unable or unwilling to serve. The form requires detailed information about the agent and alternate, including their names, addresses, and multiple contact numbers, ensuring they can be reached when needed. To establish the form’s legality, it mandates the signature of the patient, who must be at least 18 years of age or an emancipated minor, alongside the completion and signing of either Block A, which involves the authentication by two witnesses who are not related to the patient by blood, marriage, or adoption, and who would not benefit from the patient’s estate, or Block B, requiring notarization to affirm the patient’s identity, sound mind, and voluntary signature. This approval from the Tennessee Department of Health, Board for Licensing Health Care Facilities underscores the form's importance and the stringent measures in place to ensure it reflects the patient’s genuine wishes without any external pressures, fraud, or undue influence.
| Question | Answer |
|---|---|
| Form Name | Appointment Of Health Care Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | tennessee health care agent, tn health care form, appointment of health care agent, appointment care agent |
APPOINTMENT OF HEALTH CARE AGENT
(Tennessee)
I, _________________________________, give my agent named below permission to make health care
decisions for me if I cannot make decisions for myself, including any health care decision that I could have made for myself if able. If my agent is unavailable or is unable or unwilling to serve, the alternate named below will take the agent’s place.
Agent: |
Alternate: |
Name
Address
City |
State |
Zip Code |
Name
Address
City |
State |
Zip Code |
()
Area Code |
Home Phone Number |
()
Area Code |
Work Phone Number |
()
Area Code |
Mobile Phone Number |
|
|
|
|
Patient’s name (please print or type) |
Date |
|
()
Area Code |
Home Phone Number |
()
Area Code |
Work Phone Number |
()
Area Code Mobile Phone Number
Signature of patient (must be at least 18 or emancipated minor)
To be legally valid, EITHER block A OR block B must be properly completed and signed.
Block A |
Witnesses (2 witnesses required) |
|
1. I am a competent adult who is not named above. |
|
|
I witnessed the patient’s signature on this form. |
Signature of witness number 1 |
|
2. I am a competent adult who is not named above. I am not
related to the patient by blood, marriage, or adoption and I Signature of witness number 2 would not be entitled to any portion of the patient’s estate upon
his or her death under any existing will or codicil or by operation of law. I witnessed the patient’s signature on this form.
Block B |
Notarization |
STATE OF TENNESSEE
COUNTY OF
I am a Notary Public in and for the State and County named above. The person who signed this instrument is personally known to me (or proved to me on the basis of satisfactory evidence) to be the person whose name is shown above as the “patient.” The patient personally appeared before me and signed above or acknowledged the signature above as his or her own. I declare under penalty of perjury that the patient appears to be of sound mind and under no duress, fraud, or undue influence.
My commission expires:
Signature of Notary Public
Approved by Tennessee Department of Health, Board for Licensing Health Care Facilities, February 3, 2005