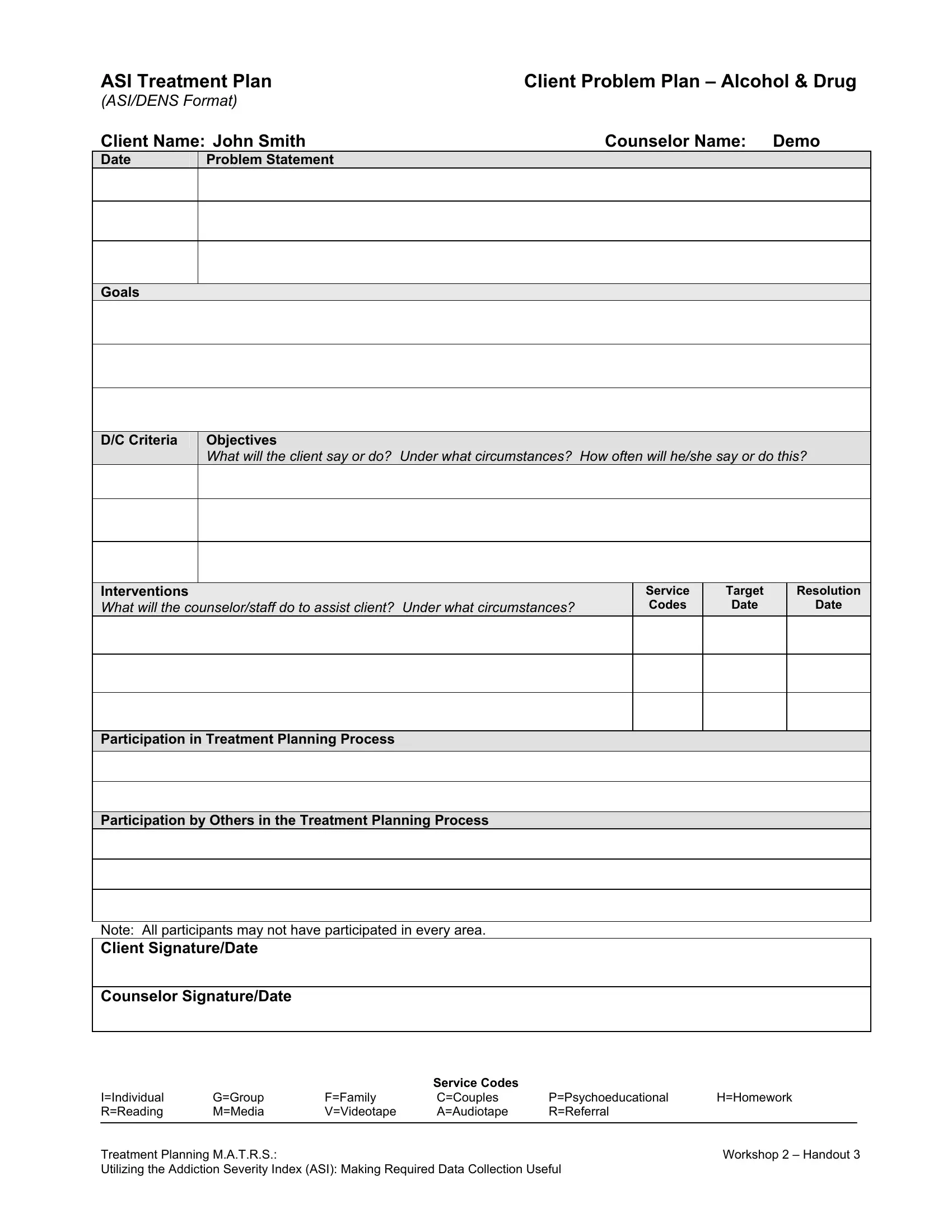
The ASI Treatment Plan is a foundational document in substance use disorder treatment and mental health recovery. It translates Addiction Severity Index scores into a structured care roadmap, covering problem statements, goals, measurable objectives, interventions, and service codes. Severity scores range from 0 to 9 per domain. Scores at 4 or higher in areas such as drug use, alcohol use, or psychiatric status indicate the need for active treatment in that domain.
Each plan is tailored to the individual client using assessment data from the Addiction Severity Index, covering all major problem domains: drug and alcohol use, medical status, employment, legal history, family relationships, and psychiatric symptoms. Objectives define what the client is expected to achieve and how frequently progress is reviewed.
Discharge criteria are documented from the start, giving both clients and counselors clear milestones for treatment completion. Client and family participation are both recorded, reinforcing accountability throughout the recovery process. For related forms, the Addiction Severity Form and Provider Treatment Plan are commonly used alongside the ASI form in clinical settings.
| Question | Answer |
|---|---|
| Form Name | Asi Treatment Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | treatment plan alcohol drug, treatment plan client alcohol, treatment plan alcohol drug template, asi treatment |