Our leading computer programmers worked hard to build the PDF editor we're content to present to you. This app will let you effortlessly prepare provider treatment plan and saves your time. You just have to stick to this procedure.
Step 1: To start with, select the orange "Get form now" button.
Step 2: You will discover all the options you can take on your file as soon as you've entered the provider treatment plan editing page.
These particular areas are going to make up the PDF document:
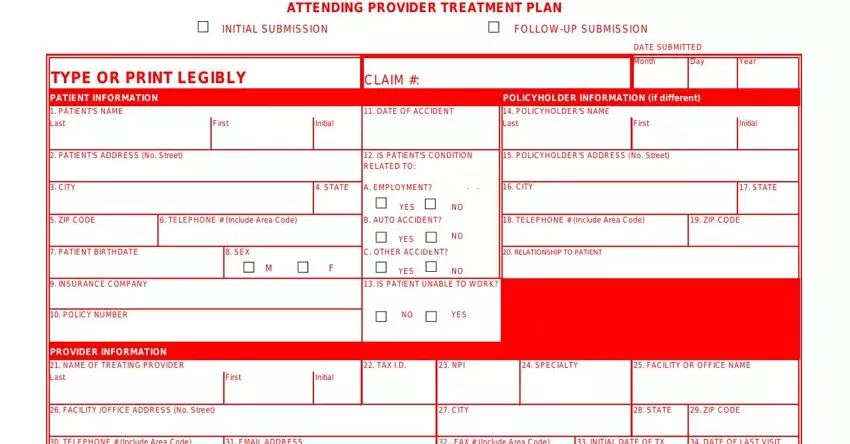
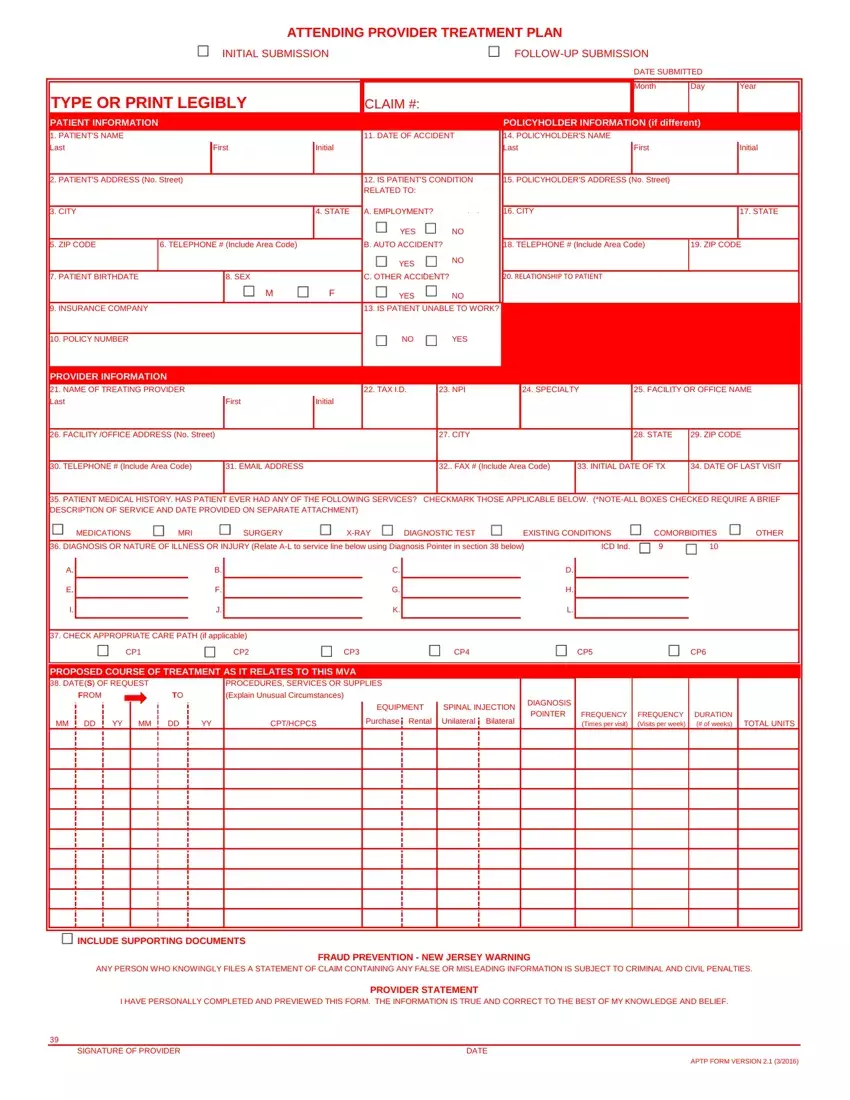
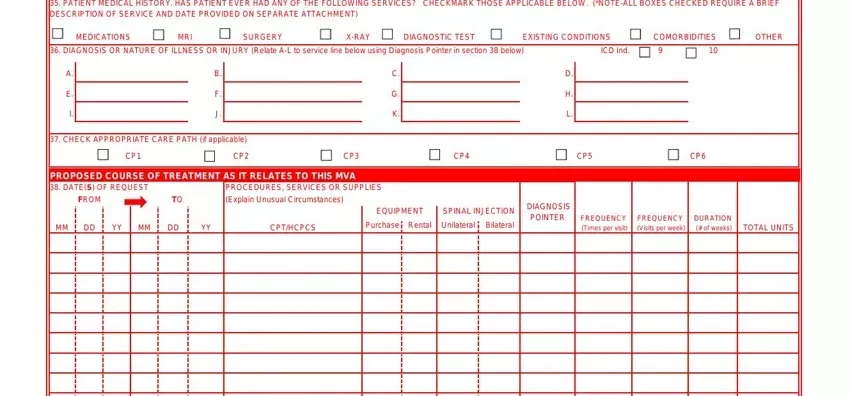
The program will expect you to complete the MEDICATIONS, MRI, SURGERY, X, RAY DIAGNOSTIC, TEST EXISTING, CONDITIONS ICD, In, d COM, OR, BIDI, TIES OTHER, FROM, CP, THC, PCS EQUIPMENT, Purchase, Rental SPINAL, INJECTION, Unilateral, Bilateral and DIAGNOSIS area.
Be sure to identify the crucial information within the INCLUDE, SUPPORTING, DOCUMENTS FRAUD, PREVENTION, NEW, JERSEY, WARNING PROVIDER, STATEMENT SIGNATURE, OF, PROVIDER DATE, and APT, P, FORM, VERSION area.
Step 3: Choose the button "Done". Your PDF file is available to be transferred. It's possible to save it to your device or email it.
Step 4: You could make duplicates of the form toavoid any possible future complications. You need not worry, we cannot distribute or check your details.
