Our main programmers worked hard to obtain the PDF editor we are pleased to present to you. Our app lets you effortlessly complete Yerawada and saves your time. You simply need to stick to the following guide.
Step 1: Click on the button "Get Form Here".
Step 2: As soon as you enter our Yerawada editing page, you will see lots of the functions it is possible to undertake regarding your form in the upper menu.
Create the Yerawada PDF and type in the material for every single segment:
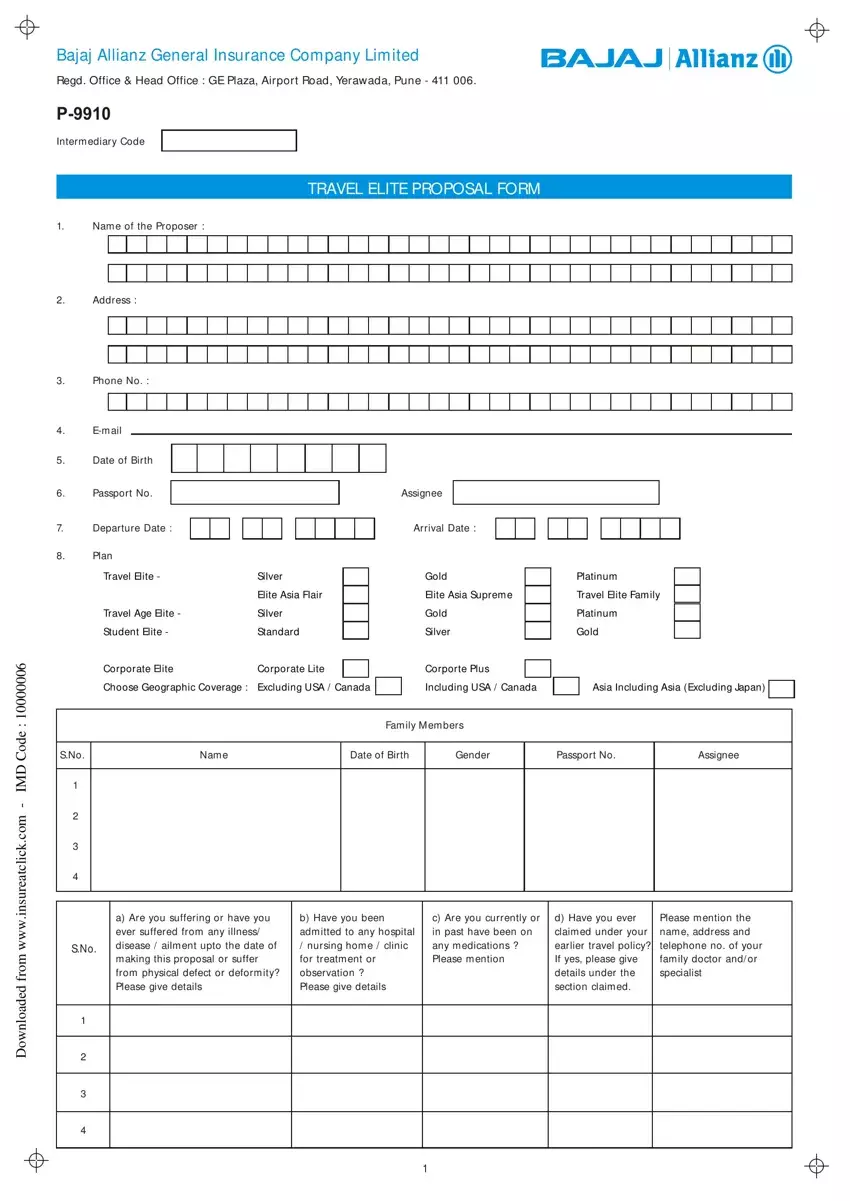
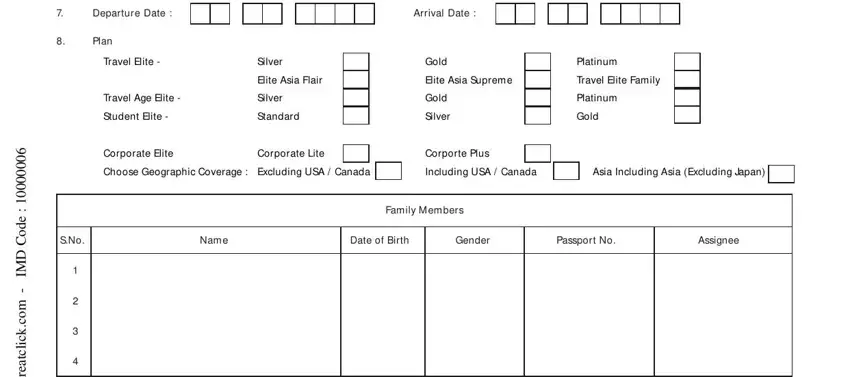
Fill in the Departure Date, Plan, Arrival Date, Travel Elite, Silver, Gold, Platinum, Elite Asia Flair, Elite Asia Supreme, Travel Elite Family, Travel Age Elite, Student Elite, Silver, Standard, and Gold areas with any data that will be required by the application.
In the area discussing a Are you suffering or have you, b Have you been admitted to any, d Have you ever claimed under your, and d e d a o l n w o D, you have got to write down some required data.
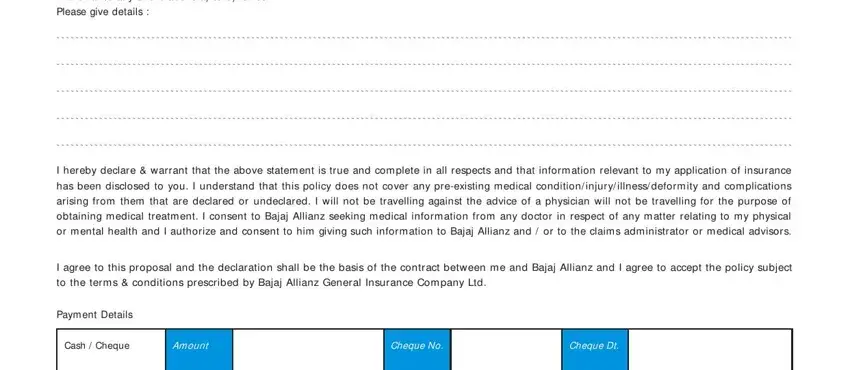
Please place the rights and responsibilities of the parties inside the If answer to any of the above a to, Please give details, I hereby declare warrant that the, has been disclosed to you I, arising from them that are, obtaining m edical treatm ent I, or m ental health and I authorize, I agree to this proposal and the, to the term s conditions, Payment Details, Cash Cheque, Amount, Cheque No, and Cheque Dt section.
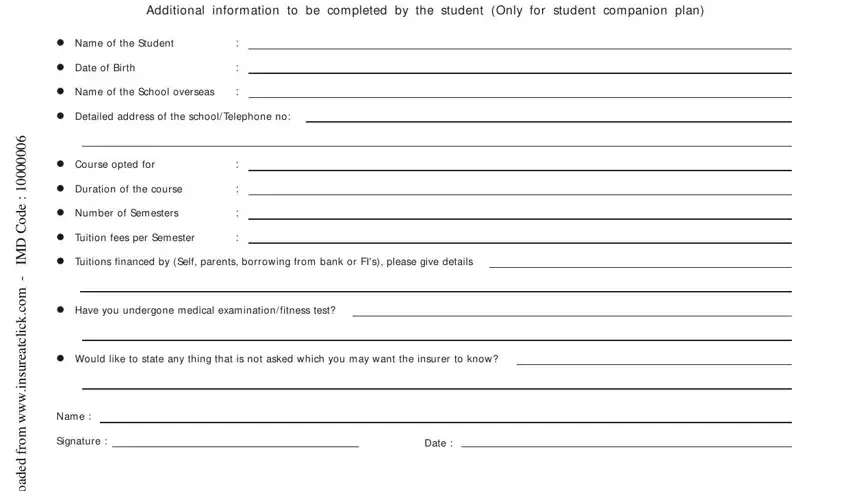
Prepare the file by checking all these areas: Additional information to be, Name of the Student, Date of Birth, Name of the School overseas, Detailed address of the school, Course opted for, Duration of the course, Number of Semesters, Tuition fees per Semester, Tuitions financed by Self parents, Have you undergone medical, Would like to state any thing that, Name, Signature, and Date.
Step 3: Hit the button "Done". Your PDF file is available to be transferred. You may obtain it to your laptop or email it.
Step 4: Be sure to get as many copies of your form as you can to stay away from potential issues.
