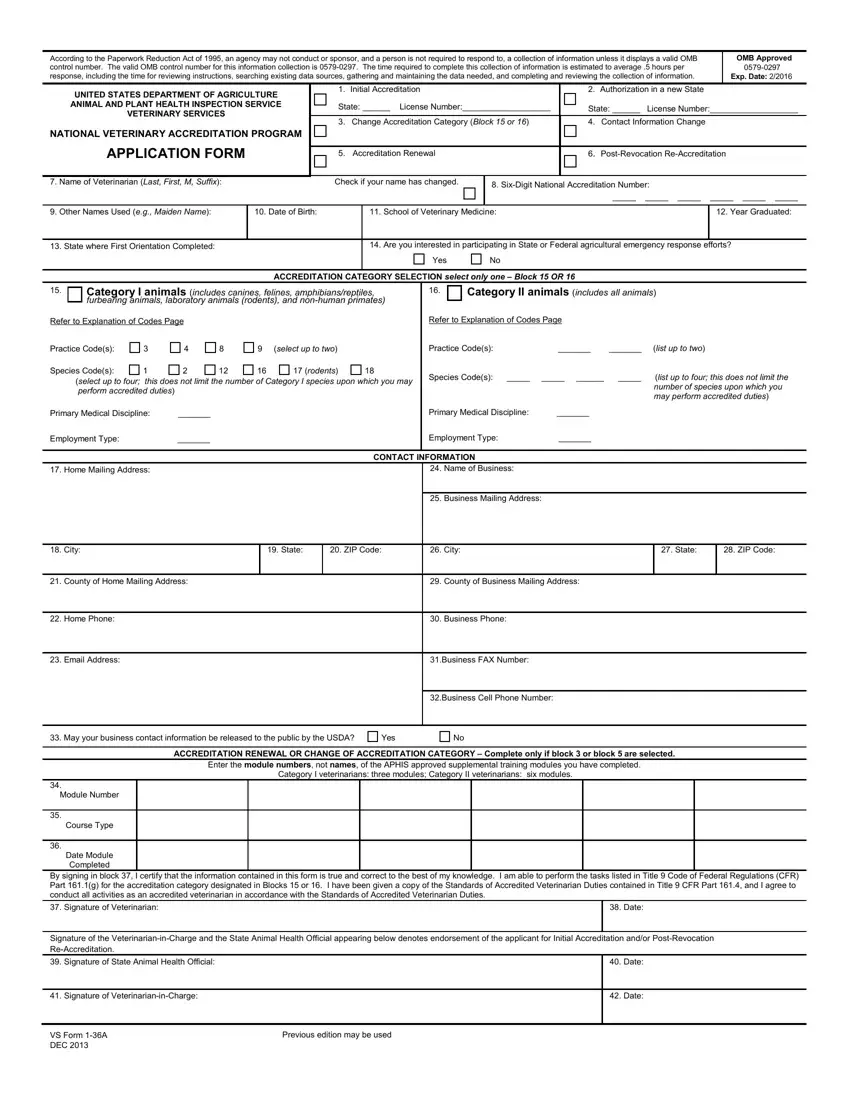
The blank MRI medical form, officially known as USDA VS Form 36A, is the primary application document for veterinarians seeking accreditation or reaccreditation through the National Veterinary Accreditation Program (NVAP). The form is authorized under OMB control number 0579-0297, in compliance with the Paperwork Reduction Act of 1995.
Veterinarians use this form for several purposes: initial NVAP accreditation, accreditation renewals, authorization to work in additional states, accreditation category changes, and contact information updates. When completing the form, you must provide personal information, educational background, accreditation category details, and contact information. The certification section requires your signature and the date, along with any required state animal health official signatures.
FormsPal also offers related veterinary and medical PDF forms, including a veterinary certificate, a veterinary travel certificate form, and an AARP medical record form.
| Question | Answer |
|---|---|
| Form Name | Blank MRI Medical Form (VS Form 36A) |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 min |
| Also known as | VS Form 36A, USDA NVAP Form, Form 36A National |
