
blood donor questionnaire uk can be completed online without difficulty. Simply make use of FormsPal PDF editing tool to perform the job without delay. To maintain our tool on the forefront of efficiency, we strive to put into operation user-oriented features and enhancements on a regular basis. We're at all times grateful for any feedback - join us in reshaping how we work with PDF forms. This is what you'd need to do to start:
Step 1: First, access the tool by pressing the "Get Form Button" in the top section of this webpage.
Step 2: With the help of this handy PDF file editor, you can do more than merely fill out forms. Edit away and make your forms appear faultless with custom textual content put in, or adjust the original input to perfection - all that comes along with an ability to add any pictures and sign the PDF off.
As for the blank fields of this particular document, this is what you want to do:
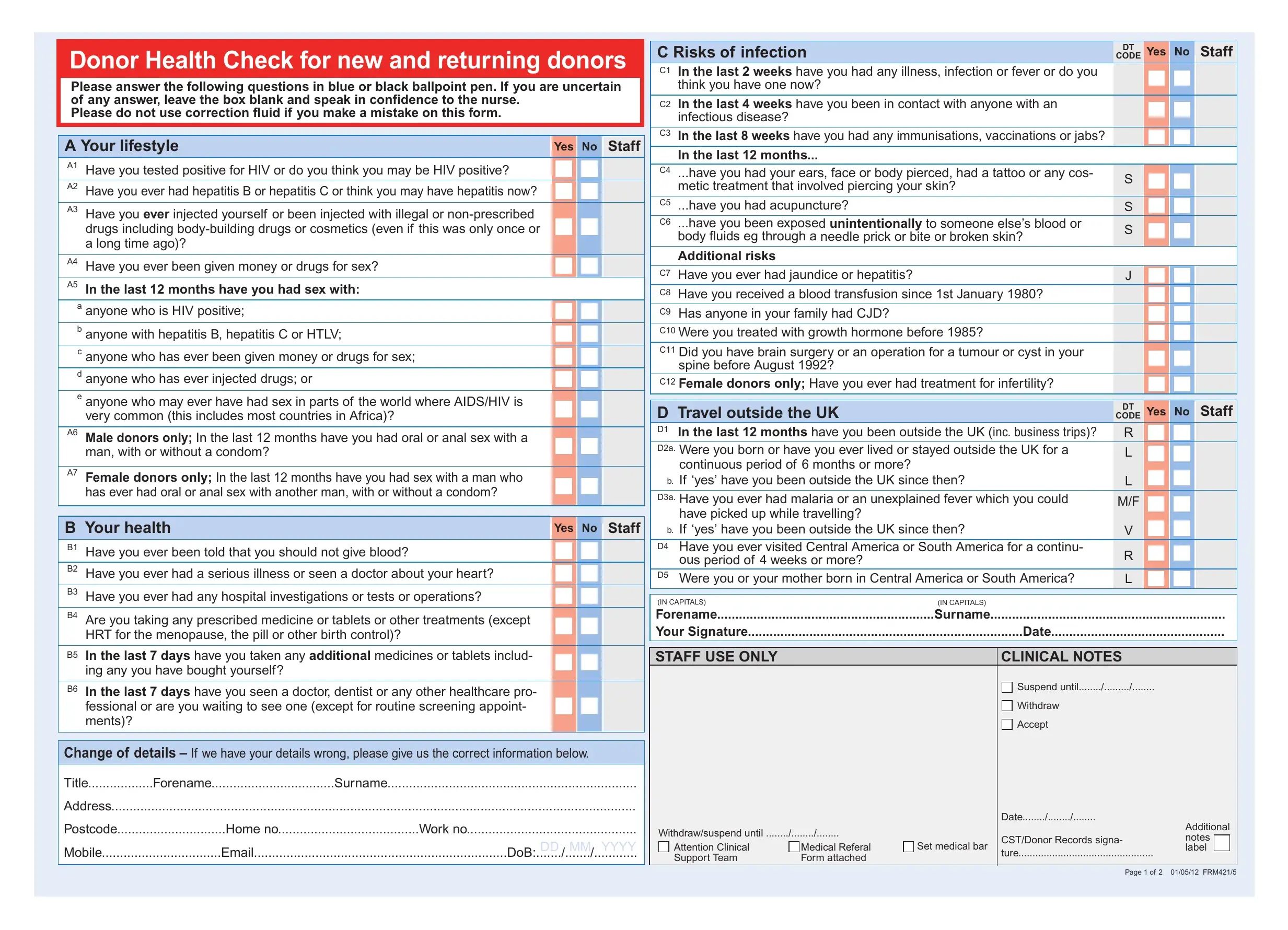
1. Complete your blood donor questionnaire uk with a group of major blanks. Gather all of the information you need and ensure there is nothing missed!
2. Right after filling in the last step, head on to the subsequent part and fill in the essential details in all these blank fields - Yes No, Staff, In the last months have you been, Have you ever had malaria or an, Were you or your mother born in, A Female donors only In the last , has ever had oral or anal sex with, B Your health B, Have you ever been told that you, Have you ever had a serious, Have you ever had any hospital, Are you taking any prescribed, IN CAPITALS ForenameSurname Your, IN CAPITALS, and B In the last days have you taken.
3. The following segment is about PostcodeHome noWork no DD MM YYYY, Withdrawsuspend until , Attention Clinical Support Team, Medical Referal Form attached, Date, Set medical bar, CSTDonor Records signa ture, Additional notes label, and Page of FRM - fill out each of these blank fields.

Concerning Attention Clinical Support Team and Set medical bar, be certain that you get them right in this current part. These could be the key fields in the page.
Step 3: Immediately after going through the fields you have filled in, hit "Done" and you are good to go! Join FormsPal right now and instantly access blood donor questionnaire uk, ready for download. All modifications made by you are kept , making it possible to change the document later on if needed. FormsPal offers safe form completion with no personal data record-keeping or distributing. Feel safe knowing that your information is safe here!