
Our PDF editor you are going to apply was made by our best software engineers. It is possible to prepare the what is a c27 form form quickly and efficiently applying our software. Simply try out this specific guide to get going.
Step 1: Choose the orange "Get Form Now" button on the webpage.
Step 2: The form editing page is presently open. You can include information or manage existing details.
Create the what is a c27 form PDF and enter the content for every single area:
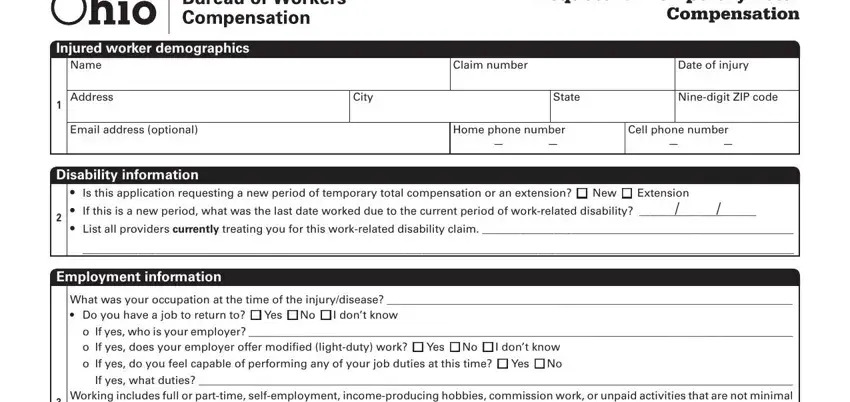
Jot down the details in If yes what duties Working, o If yes who is your employer, Have you previously worked in any, o If yes who is your employer o, Vocational rehabilitation, Vocational rehabilitation is an, Benefitsearnings received or, Receiving Beginning date of benefit, Type of benefit Unemployment If yes, n Yes n No n Yes n No n Yes n No, n Yes n No, Wagesalary continuation If yes, n Yes n No, and n Yes n No.
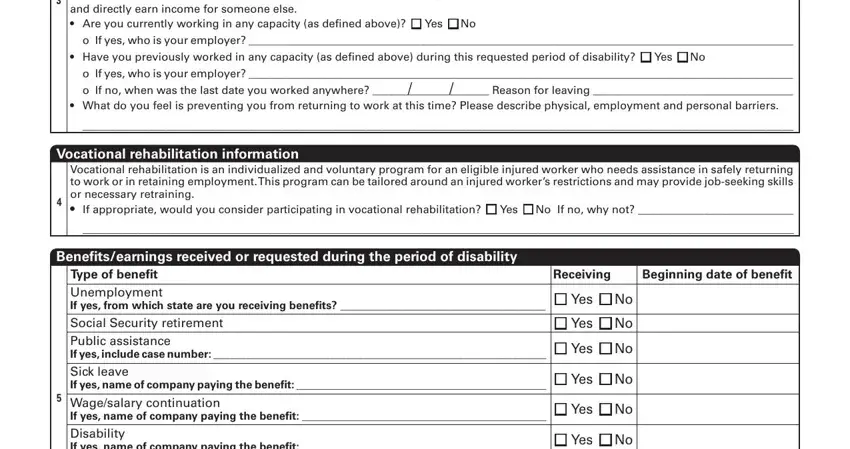
Highlight the most important details of the Wagesalary continuation If yes, Earnings to include full or part, n Yes n No, Injured worker signature, I understand I am not permitted to, Date, and C BWC Rev March field.
Step 3: Press the button "Done". The PDF form is available to be transferred. You can easily obtain it to your laptop or send it by email.
Step 4: Have at least two or three copies of the form to avoid all of the possible future troubles.
