
 Yes
Yes  No If yes, provide the date patient reached MMI: _____/_____/_____
No If yes, provide the date patient reached MMI: _____/_____/_____ Yes
Yes  No
No
 C-4.3
C-4.3
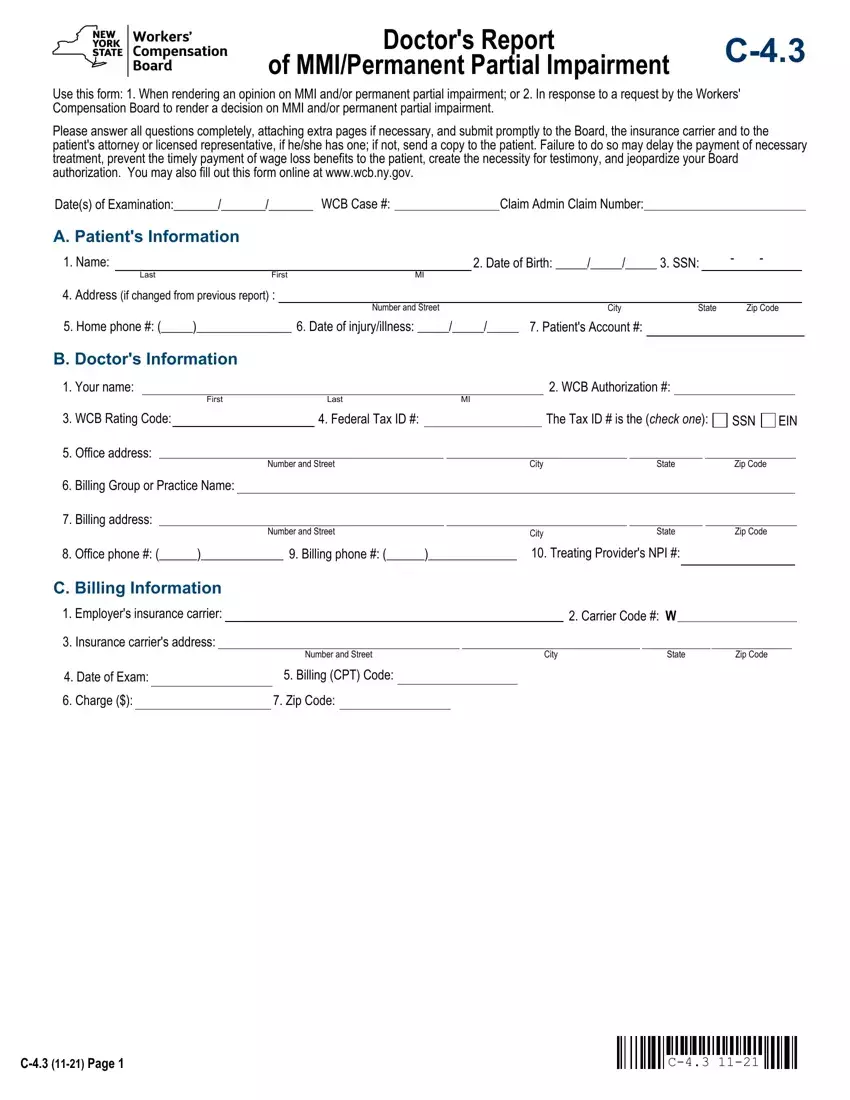
The ny c4 3 form filling out course of action is quick. Our software lets you use any PDF form.
Step 1: Look for the button "Get Form Here" on this website and press it.
Step 2: Now you will be on the file edit page. It's possible to add, customize, highlight, check, cross, include or delete fields or text.
Feel free to enter the next information to complete the ny c4 3 form PDF:
The system will need you to fill in the C Billing Information, Employers insurance carrier, Insurance carriers address, Date of Exam, Charge, Number and Street, Billing CPT Code, Zip Code, Carrier Code W, City, State, and Zip Code part.
Note the key information in C Page section.

The Patients Name, Last First MI, Date of injuryonset of illness, D Maximum Medical Improvement, Has the patient reached Maximum, Yes, If yes provide the date patient, If No describe why the patient has, E Permanent Partial Impairment, Is there permanent partial, Yes, and List the body parts and field is where both parties can put their rights and responsibilities.
End up by reviewing all these fields and preparing them accordingly: This form is signed under penalty, Name, Signature, Specialty, Date, and C Page.

Step 3: Hit the "Done" button. Now you may export your PDF document to your gadget. Additionally, you may deliver it via email.
Step 4: You can generate duplicates of your file tokeep clear of different potential future worries. You should not worry, we don't distribute or check your information.
