Completing the C-11 employment status change form is simple with our free PDF editor. Use the steps below to fill out all required fields, sign the form, and download your completed copy.
Step 1: Click "Get Form Here" on this page to open the C-11 in our free online editor and access all available editing tools.
Step 2: Once on the editing page, you will see all available free editing tools in the top menu. Use these to complete each required field. Check each section for accuracy before continuing.
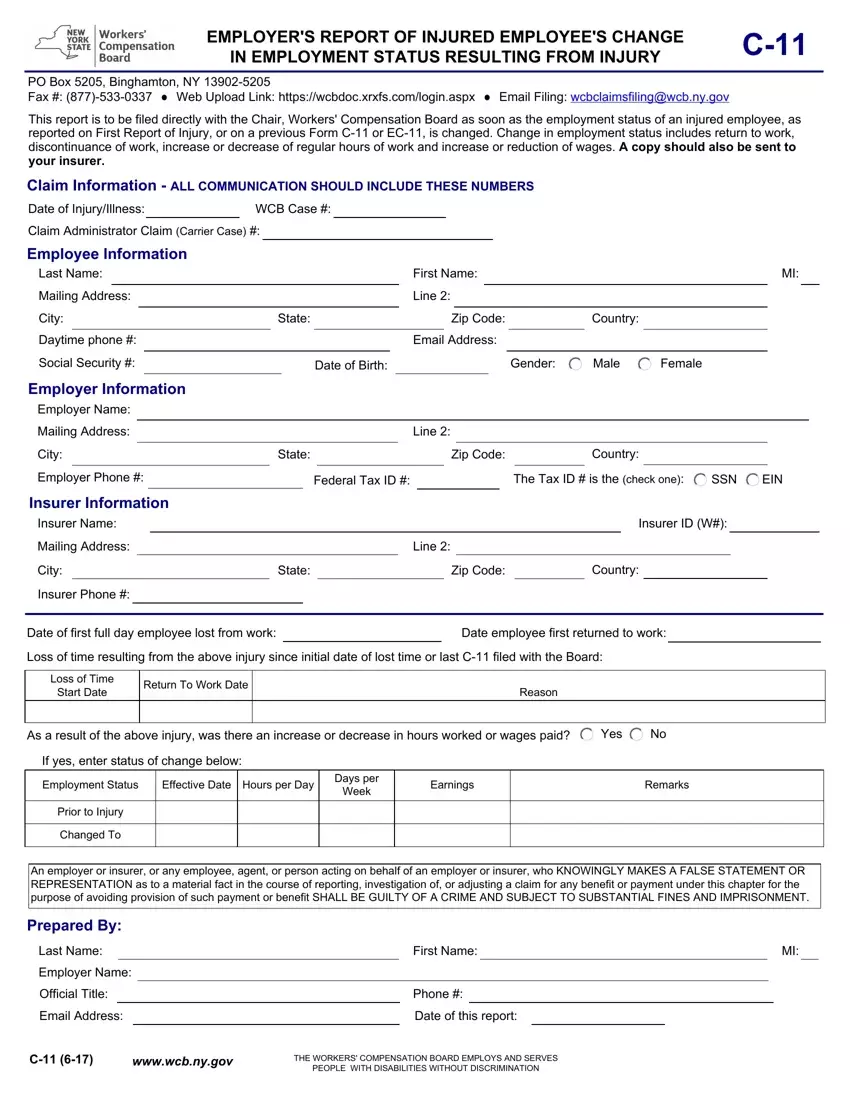
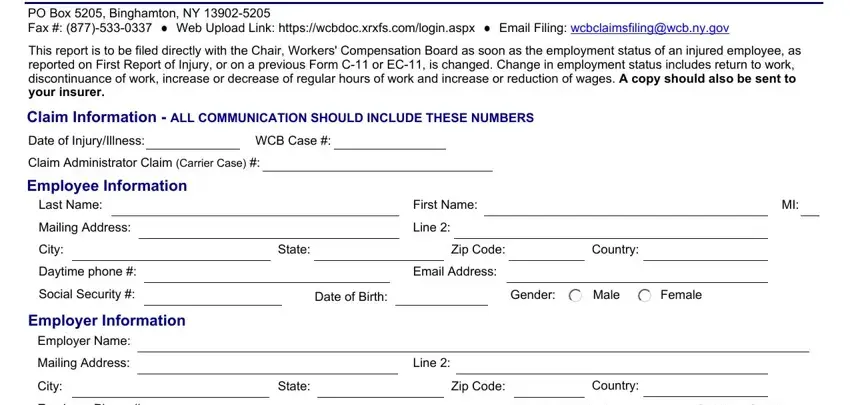
For each section, enter the information requested.
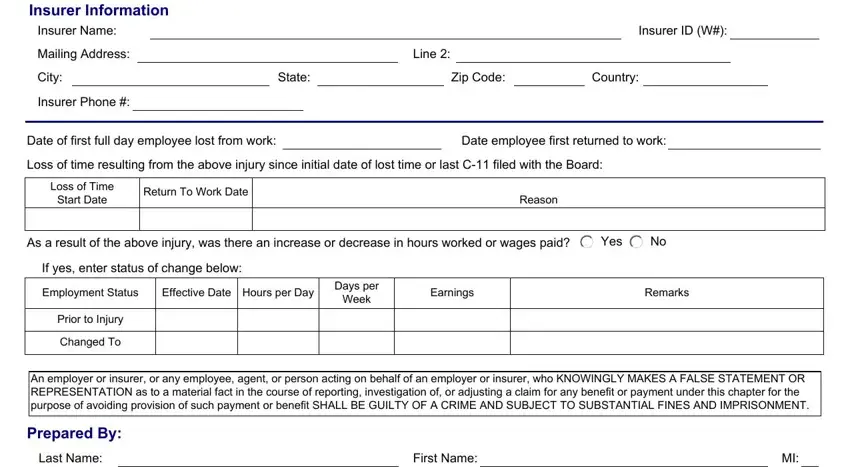
In the Insurer Information section: enter Insurer Name, Mailing Address, City, Phone, State, Zip Code, Country, and Insurer ID. Also enter the Date of first full day unable to work, Date the employee first returned to work, Loss of Time Start Date, Return To Work Date, and Loss of Time information. Updated dates and accurate wage documents are required for compliance.
In the Employer section: enter Employer Name, Title, Email, Phone, Date of this form, and WCB case details. Complete the WCB section fields as indicated. The form must be signed by an authorized employer representative before submission.

Step 3: Click Done to save the completed form. You can then download, export, or print the free form directly. Check the completed form before saving to confirm all fields are accurate.
Step 4: Make several copies. New York employers must send one copy to the New York WCB and one to the workers compensation insurance policy carrier. Keep signed copies within your business records for compliance and government documentation purposes.
Frequently Asked Questions
Employers often have questions about C-11 form filing requirements. The answers below address the most common concerns about submission timelines, required documentation, and how to access free forms and resources through the WCB website and FormsPal.
What is the C-11 form used for in New York?
The C-11, officially the Employer's Report of Injured Employee's Change in Employment Status, is a workers compensation form used by New York employers to notify the WCB of any employment status update involving an injured worker. This includes a return to work, stopping work, or a change in wages or hours. Timely filing is required for compliance with New York employer regulations. Contact the WCB or access employer resources for additional guidance.
Are these free forms available online?
Yes. The C-11 and other free New York employer forms on FormsPal are free to access, fill out, and download. Use the free PDF editor to complete the form, then download or print at no cost. No sign-up is required to access free forms on FormsPal. Users can also search for and explore other required employer forms. Contact our support team for user assistance.
Where do I submit the completed C-11 form?
Submit the completed form to the New York WCB via fax, web upload, or email. Also send a copy to your workers compensation insurance policy carrier. Contact the WCB directly to confirm submission details, contact information, and required documents. Filing employer forms promptly after any employment status update is required for compliance with WCB regulations. Continue to track your employment documentation within the required timeframe.
What situations require filing a new C-11?
File a new C-11 after any employment status update since the last submission. This includes a return to work in any capacity (full-time, part-time, or modified duty), stopping work, wage changes, or hour changes. New York employers must continue to submit the required free forms promptly after each status update throughout the claim. Contact the WCB if you need additional government guidance, and explore safety and compliance resources within the required timeframe.
How do I document lost wages on the C-11 form?
The C-11 asks employers to report whether the injured worker experienced any lost wages following the date of injury. Enter the loss of time start date, the return-to-work date, and current wage data in the appropriate fields. For wage changes spanning multiple pay periods, use the Employer Wage Verification Form to support the filing. Accurate reporting of lost wages ensures the injured worker receives correct wage replacement benefits and protects your business from compliance penalties. Contact your workers compensation carrier or the WCB for additional guidance on wage reporting requirements.
