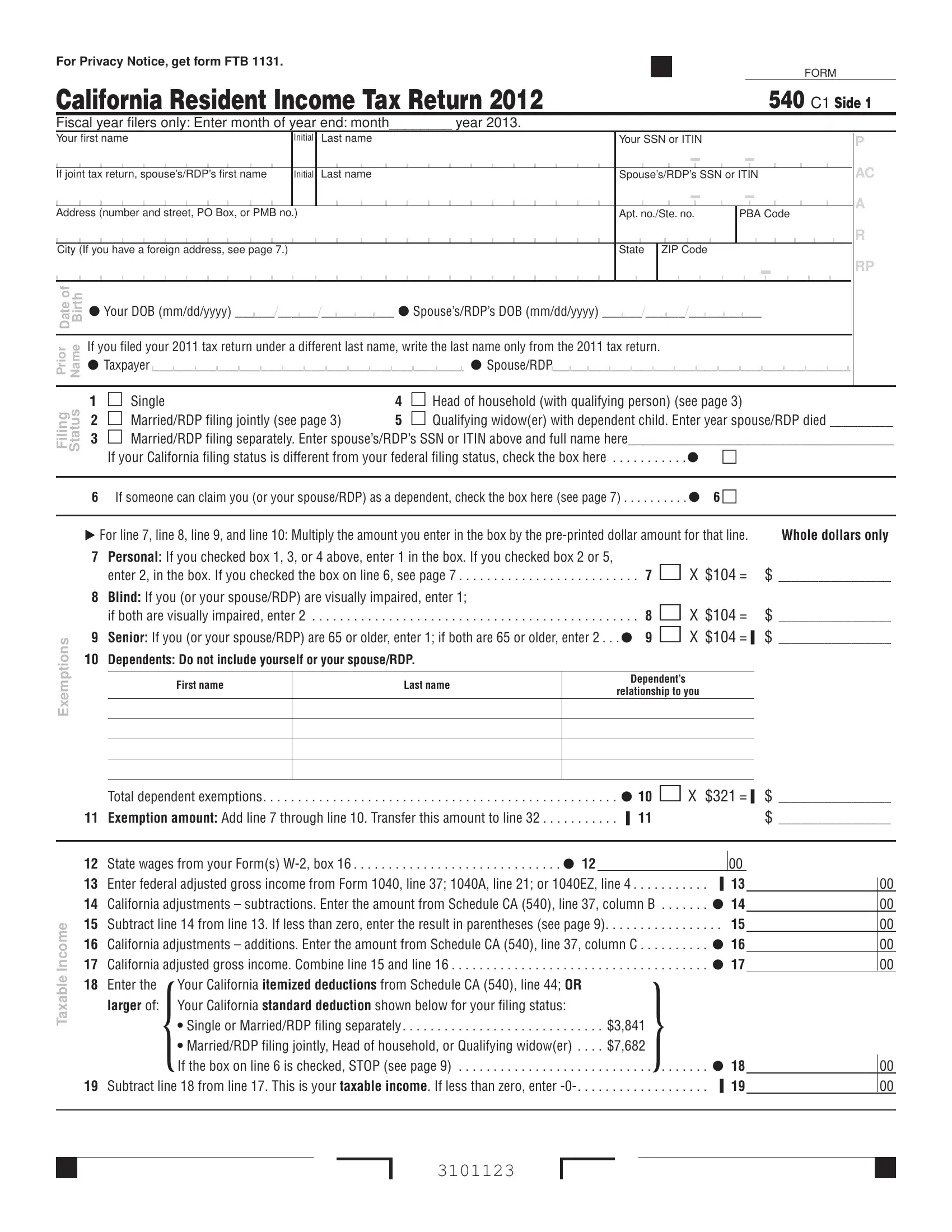
California Form 540 C1 is the 2012 Resident Income Tax Return filed with the California Franchise Tax Board (FTB). California residents and registered domestic partners (RDPs) use this tax form to report income, claim deductions and credits, and calculate the California taxes owed or refund due for the 2012 tax year.
The form covers all major areas of California income tax filing:
Mail the completed Form 540 C1 and any balance due to the Franchise Tax Board at the mailing address shown at the bottom of the return. Keep copies of all California tax forms, W-2 statements, and supporting documents for your records.
| Question | Answer |
|---|---|
| Form Name | California Form 540 C1 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | 540 fillable form, ca ftb 540 instructions, 540 form, ITIN |