
California Form Dhs 4516 can be filled in online in no time. Just open FormsPal PDF editor to get it done without delay. The editor is continually updated by our team, receiving new features and becoming better. Should you be seeking to start, here's what it will take:
Step 1: Simply press the "Get Form Button" at the top of this page to see our pdf editor. Here you will find everything that is necessary to fill out your file.
Step 2: With our online PDF file editor, you can actually do more than merely fill out blank fields. Express yourself and make your docs appear professional with custom textual content added in, or optimize the file's original content to excellence - all that comes with an ability to insert stunning images and sign the file off.
This PDF doc requires some specific details; in order to guarantee correctness, please make sure to pay attention to the tips further on:
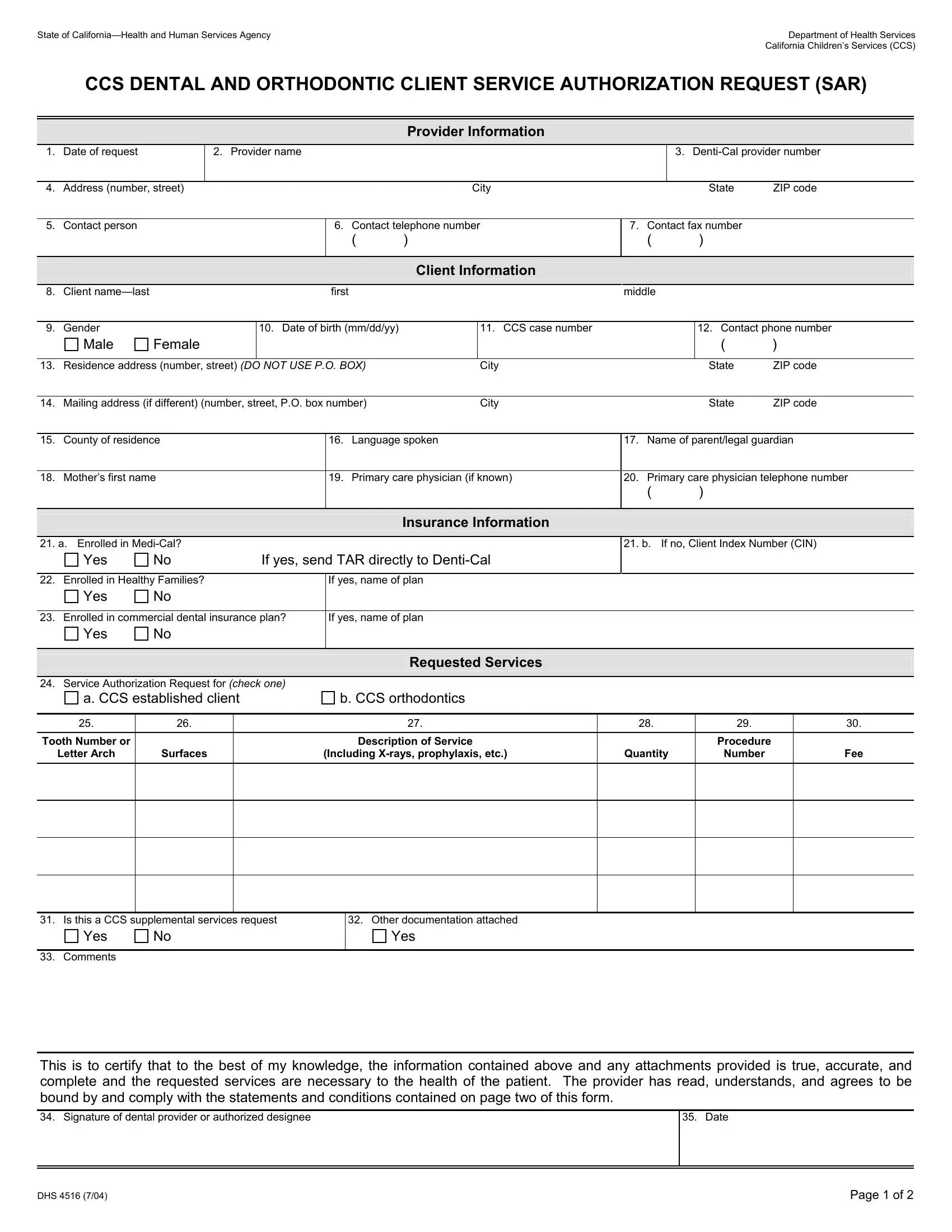
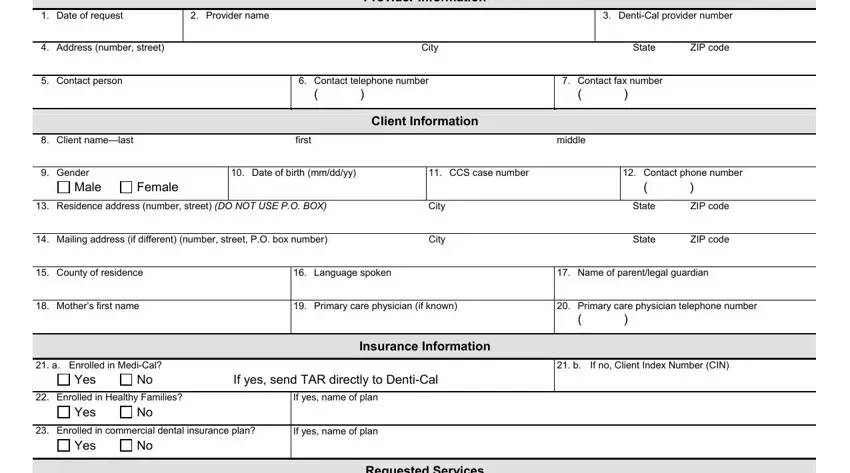
1. Before anything else, while completing the California Form Dhs 4516, begin with the part that features the next blanks:
2. After this part is done, go on to type in the suitable information in all these - Service Authorization Request for, a CCS established client, b CCS orthodontics, Requested Services, Tooth Number or, Letter Arch, Surfaces, Description of Service, Including Xrays prophylaxis etc, Quantity, Procedure, Number, Fee, Is this a CCS supplemental, and Other documentation attached.
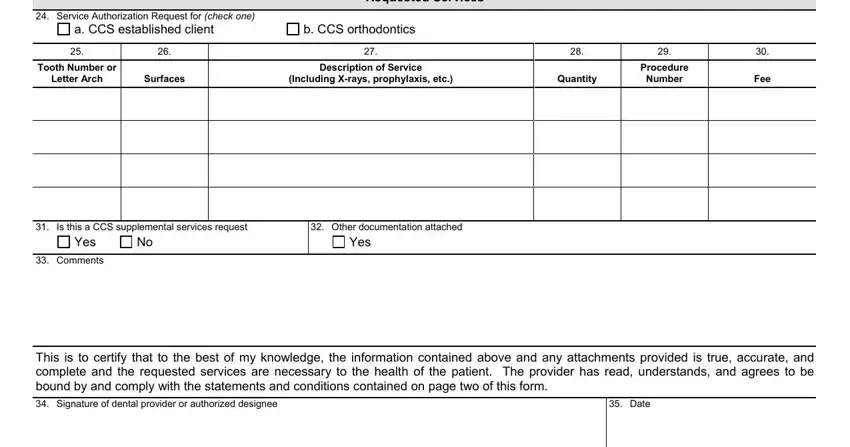
Regarding Procedure and Other documentation attached, make sure you double-check them here. Both these are considered the most important ones in this page.
Step 3: Right after rereading the filled out blanks, click "Done" and you are good to go! Join FormsPal today and immediately obtain California Form Dhs 4516, prepared for downloading. All adjustments made by you are saved , meaning you can modify the form at a later stage if required. At FormsPal.com, we strive to ensure that your information is kept protected.