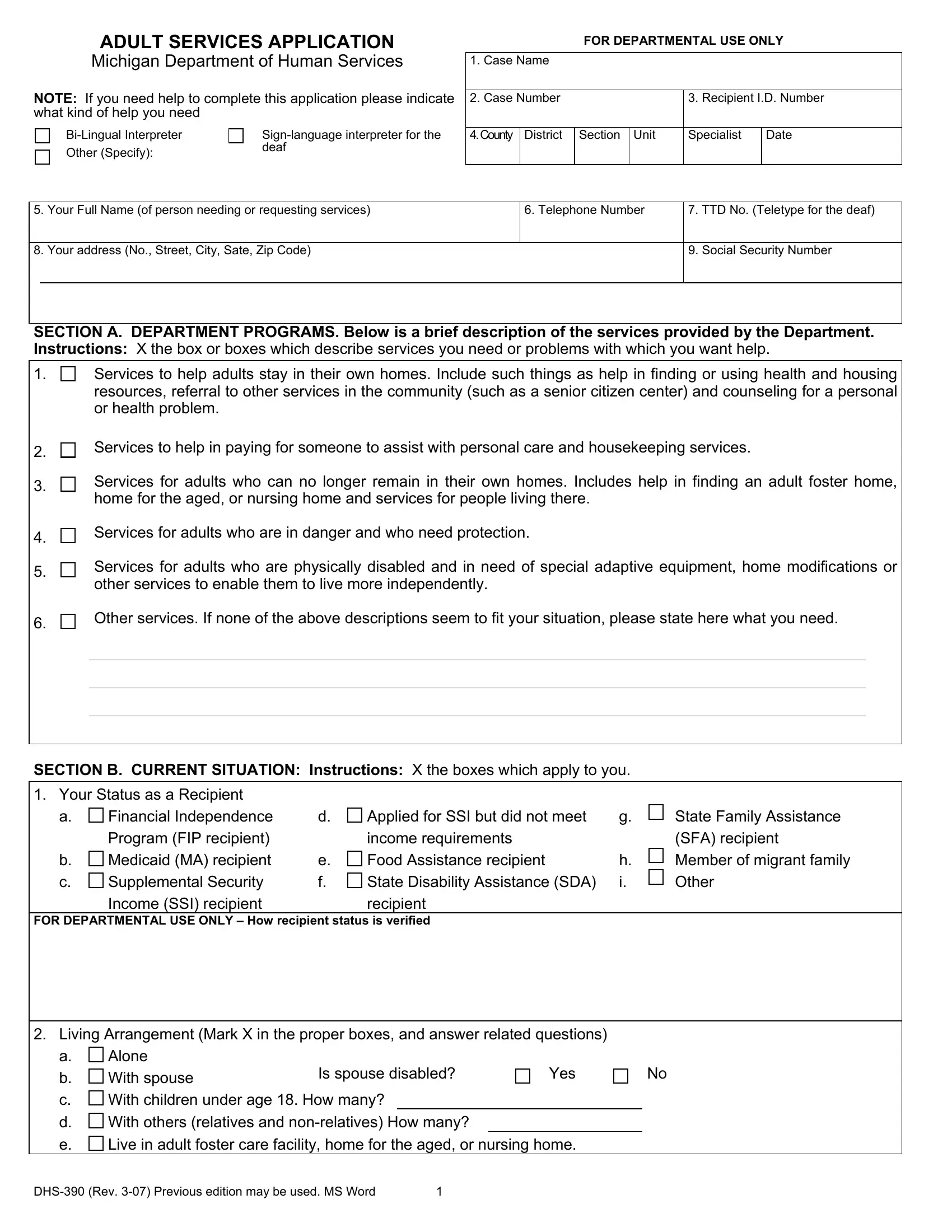
The DHS 390 form, an integral document from the Michigan Department of Human Services, serves as an application for a wide range of adult services intended to enhance the well-being and independence of applicants. This comprehensive application process is designed to address the needs of adults seeking assistance to remain in their homes, require help with personal care and housekeeping, or need protection due to being in danger. Additionally, it encompasses services for adults who cannot stay in their homes anymore by facilitating the search for adult foster care, homes for the aged, or nursing facilities, as well as providing support for those already residing in such institutions. The form is also tailored to assist physically disabled adults in acquiring special adaptive equipment or home modifications to live more independently. Significantly, the DHS 390 form stands as a testament to the commitment of the Michigan Department of Human Services to ensure that every individual is treated with fairness, dignity, and without discrimination, emphasizing the rights of applicants to a prompt review process, non-discrimination, and the ability to appeal decisions. Furthermore, responsibilities of the applicants, such as providing accurate information and promptly reporting changes in their situation, are clearly outlined, ensuring a mutual understanding between the Department and the service beneficiaries.
| Question | Answer |
|---|---|
| Form Name | Form Dhs 390 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Sate, NONDISCRIMINATION, dhs 390 form, TTD |
