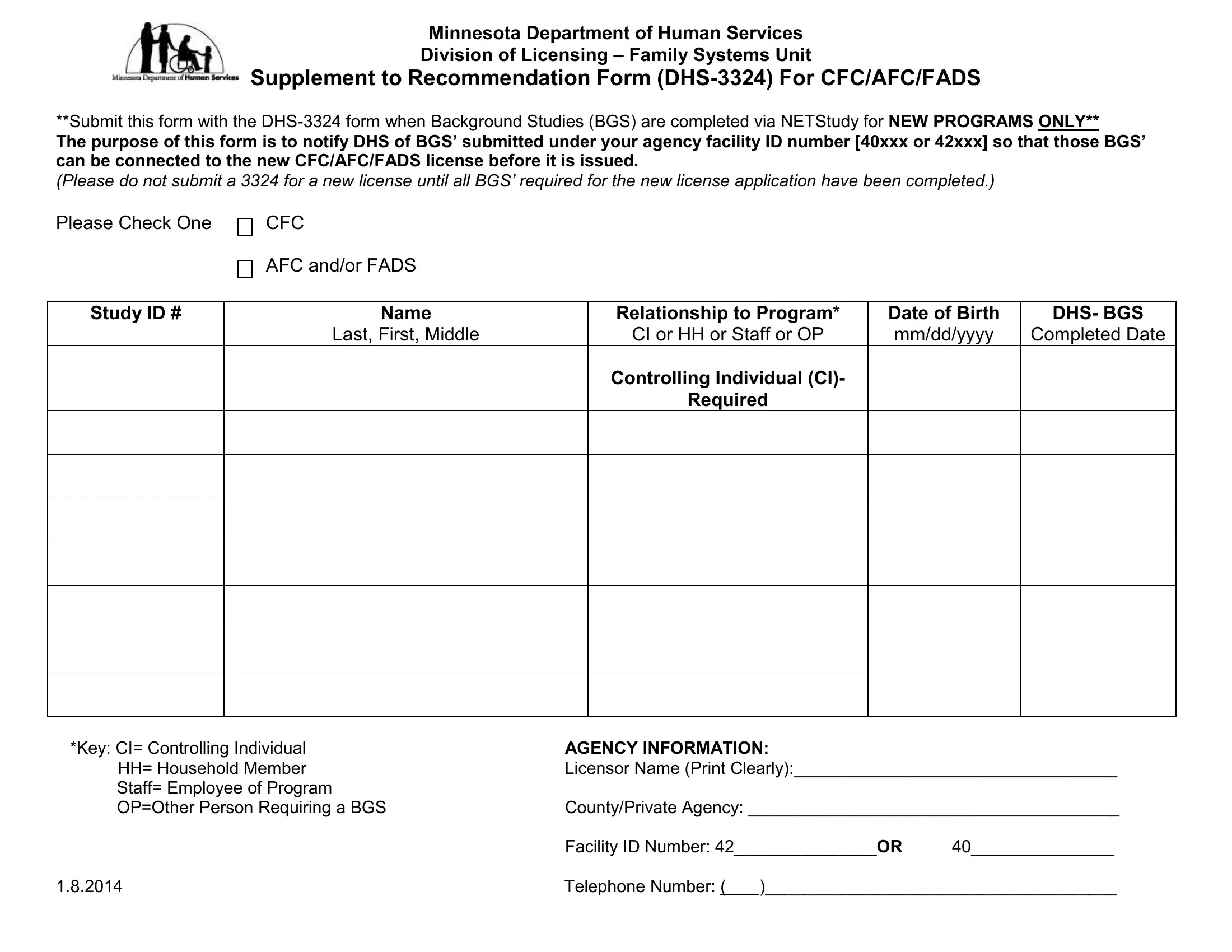
Understanding the complexities and nuances of the DHS-3324 form is crucial for anyone involved in the operations of new Community Residential Settings (CFC), Adult Foster Care (AFC), or Family Adult Day Services (FADS) programs within Minnesota. This Supplement to Recommendation Form, issued by the Minnesota Department of Human Services Division of Licensing – Family Systems Unit, plays a vital role in the initial phases of licensing. Its purpose is decidedly focused on ensuring that all Background Studies (BGS) submitted by an agency under a specific facility ID number are duly connected to the pending license for new programs. It's important to highlight that this form should only be submitted after all required BGS for a new license application are completed. This form not only facilitates a smoother licensing process by notifying the Department of Human Services (DHS) about the completion of necessary background checks but also delineates the roles of various individuals involved in the program, including Controlling Individuals (CI), Household Members (HH), staff, and other persons who have undergone background studies. By providing agency and contact information upfront, it ensures a direct line of communication between the agency and the licensing unit, streamlining administrative processes and helping to expedite the final approval of the new license.
| Question | Answer |
|---|---|
| Form Name | Form Dhs 3324 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | mn dhs, mn dhs 3324 license, dhs, mn dhs foster care 3324 |
